Sarah Cullivan, Leon Genecand, Natalia El-Merhie, Alison MacKenzie, Mona Lichtblau
{"title":"Inhaled treprostinil in group 3 pulmonary hypertension associated with lung disease: results of the INCREASE and PERFECT studies.","authors":"Sarah Cullivan, Leon Genecand, Natalia El-Merhie, Alison MacKenzie, Mona Lichtblau","doi":"10.1183/20734735.0242-2024","DOIUrl":null,"url":null,"abstract":"<p><p>Group 3 pulmonary hypertension (PH) associated with lung disease is a common cause of PH and is associated with substantial morbidity and mortality. Multiple studies of pulmonary arterial hypertension (PAH) therapies in this population have demonstrated conflicting results regarding their safety and efficacy, and therefore the optimum treatment for this group is unknown. The INCREASE and PERFECT randomised, double-blind, placebo-controlled trials attempted to address this unmet need by exploring the role of inhaled treprostinil (iTRE) in PH associated with interstitial lung disease (PH-ILD) and PH associated with COPD (PH-COPD), respectively. In the INCREASE and PERFECT studies individuals were randomised to placebo or iTRE, which was administered <i>via</i> an ultrasonic, pulsed-delivery nebuliser to a maximum dose of 72 μg, four times a day. The INCREASE study randomised 326 subjects with PH-ILD over a 16-week period and met its primary endpoint of change in 6-min walk distance, with a treatment effect of +31.12 m (p<0.001). Reduced disease progression events and increased forced vital capacity were also reported in the treatment arm in a <i>post hoc</i> analysis. By contrast, the PERFECT study was stopped prematurely by the data and safety monitoring committee due to evidence that iTRE increased serious adverse events in subjects with PH-COPD. This journal club provides an overview of these important trials and highlights pertinent unanswered questions in this field.</p>","PeriodicalId":9292,"journal":{"name":"Breathe","volume":"21 1","pages":"240242"},"PeriodicalIF":3.4000,"publicationDate":"2025-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915125/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breathe","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1183/20734735.0242-2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
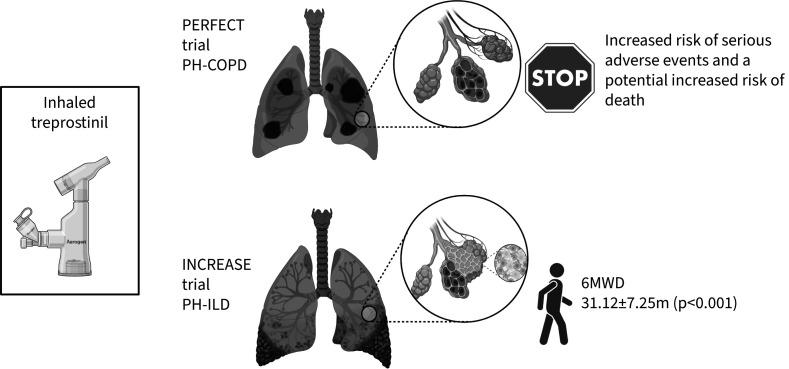
Group 3 pulmonary hypertension (PH) associated with lung disease is a common cause of PH and is associated with substantial morbidity and mortality. Multiple studies of pulmonary arterial hypertension (PAH) therapies in this population have demonstrated conflicting results regarding their safety and efficacy, and therefore the optimum treatment for this group is unknown. The INCREASE and PERFECT randomised, double-blind, placebo-controlled trials attempted to address this unmet need by exploring the role of inhaled treprostinil (iTRE) in PH associated with interstitial lung disease (PH-ILD) and PH associated with COPD (PH-COPD), respectively. In the INCREASE and PERFECT studies individuals were randomised to placebo or iTRE, which was administered via an ultrasonic, pulsed-delivery nebuliser to a maximum dose of 72 μg, four times a day. The INCREASE study randomised 326 subjects with PH-ILD over a 16-week period and met its primary endpoint of change in 6-min walk distance, with a treatment effect of +31.12 m (p<0.001). Reduced disease progression events and increased forced vital capacity were also reported in the treatment arm in a post hoc analysis. By contrast, the PERFECT study was stopped prematurely by the data and safety monitoring committee due to evidence that iTRE increased serious adverse events in subjects with PH-COPD. This journal club provides an overview of these important trials and highlights pertinent unanswered questions in this field.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
