Milena Engelke, Laura Basso, Berthold Langguth, Florian Zeman, Winfried Schlee, Stefan Schoisswohl, Rilana Cima, Dimitris Kikidis, Jose Antonio Lopez-Escamez, Petra Brüggemann, Birgit Mazurek, Jorge Piano Simões
{"title":"Estimation of Minimal Clinically Important Difference for Tinnitus Handicap Inventory and Tinnitus Functional Index.","authors":"Milena Engelke, Laura Basso, Berthold Langguth, Florian Zeman, Winfried Schlee, Stefan Schoisswohl, Rilana Cima, Dimitris Kikidis, Jose Antonio Lopez-Escamez, Petra Brüggemann, Birgit Mazurek, Jorge Piano Simões","doi":"10.1002/ohn.1217","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The minimal clinically important difference (MCID) represents the smallest change in treatment outcome deemed clinically meaningful. This study estimates the MCID for 2 widely used tinnitus measures: the Tinnitus Handicap Inventory (THI) and the Tinnitus Functional Index (TFI), using anchor-based approaches while accounting for baseline severity and time interval.</p><p><strong>Study design: </strong>A multi-center randomized clinical trial.</p><p><strong>Setting: </strong>European tinnitus centers.</p><p><strong>Methods: </strong>Anchor-based approaches, including the effect size, receiver-operating characteristics, and ΔTHI/TFI methods, were employed to determine the MCID. The \"minimally improved\" category of the Clinical Global Impression Scale-Improvement (CGI-I) served as the anchor. The standard error of measurement was used to assess random variation.</p><p><strong>Results: </strong>For the THI, MCID estimates ranged from 7.8 to 12, with a point estimate of 11 after 12 weeks of treatment (N = 364). For the TFI, MCID estimates ranged from 7.3 to 9.4, with a point estimate of 9 points after 12 weeks (N = 359). Both measures indicated that higher baseline severity and longer time intervals required greater score reduction for clinical relevance.</p><p><strong>Conclusion: </strong>This study highlights the context-specific nature of MCID values for tinnitus measures and emphasizes the need for consensus on optimal anchor-based approaches to improve comparability.</p>","PeriodicalId":19707,"journal":{"name":"Otolaryngology- Head and Neck Surgery","volume":" ","pages":"69-79"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12207346/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Otolaryngology- Head and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ohn.1217","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The minimal clinically important difference (MCID) represents the smallest change in treatment outcome deemed clinically meaningful. This study estimates the MCID for 2 widely used tinnitus measures: the Tinnitus Handicap Inventory (THI) and the Tinnitus Functional Index (TFI), using anchor-based approaches while accounting for baseline severity and time interval.
Study design: A multi-center randomized clinical trial.
Setting: European tinnitus centers.
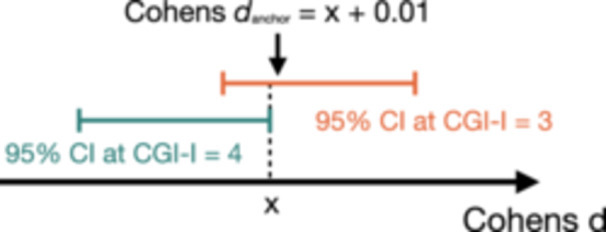
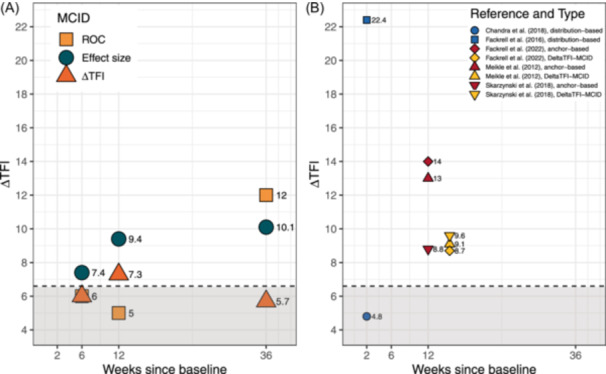
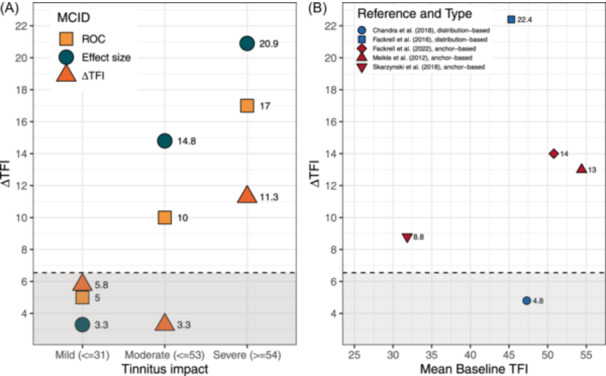
Methods: Anchor-based approaches, including the effect size, receiver-operating characteristics, and ΔTHI/TFI methods, were employed to determine the MCID. The "minimally improved" category of the Clinical Global Impression Scale-Improvement (CGI-I) served as the anchor. The standard error of measurement was used to assess random variation.
Results: For the THI, MCID estimates ranged from 7.8 to 12, with a point estimate of 11 after 12 weeks of treatment (N = 364). For the TFI, MCID estimates ranged from 7.3 to 9.4, with a point estimate of 9 points after 12 weeks (N = 359). Both measures indicated that higher baseline severity and longer time intervals required greater score reduction for clinical relevance.
Conclusion: This study highlights the context-specific nature of MCID values for tinnitus measures and emphasizes the need for consensus on optimal anchor-based approaches to improve comparability.
期刊介绍:
Otolaryngology–Head and Neck Surgery (OTO-HNS) is the official peer-reviewed publication of the American Academy of Otolaryngology–Head and Neck Surgery Foundation. The mission of Otolaryngology–Head and Neck Surgery is to publish contemporary, ethical, clinically relevant information in otolaryngology, head and neck surgery (ear, nose, throat, head, and neck disorders) that can be used by otolaryngologists, clinicians, scientists, and specialists to improve patient care and public health.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
