{"title":"Predictive factors of permanent versus transient congenital hypothyroidism: a pragmatic cohort study.","authors":"Niki Dermitzaki, Vasileios Giapros, Marianna Deligeorgopoulou, Vasiliki Rengina Tsinopoulou, Eleni Kotanidou, Maria Baltogianni, Foteini Balomenou, Anastasios Serbis","doi":"10.6065/apem.2448126.063","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To identify clinical predictors of permanent congenital hypothyroidism (PCH) and transient congenital hypothyroidism (TCH).</p><p><strong>Methods: </strong>This retrospective cohort study enrolled neonates with risk factors for congenital hypothyroidism as diagnosed by neonatal screening test or blood testing. Levothyroxine (LT4) dose and serum thyroid stimulating hormone (TSH) concentrations were recorded from birth to 3 years of age.</p><p><strong>Results: </strong>We enrolled 88 neonates, 35 with PCH and 53 with TCH. An LT4 dose > 3.8 μg/kg/day at 6 months (sensitivity 62%, specificity 96%), 3.0 μg/kg/day at 12 months (64%, 97%, respectively), 2.6 μg/kg/day at 2 years (80%, 98%), and 2.5 μg/kg/day at 3 years (89%, 98%) of age could predict PCH. Daily total LT4 doses > 50 µg at any time during the follow-up period were found solely in the PCH group (28% vs 0%, P<0.001). Independent discriminative predictors of PCH and TCH were TSH concentrations at diagnosis (beta=-4.3, P<0.001); daily LT4 dose at 6 (beta=-2.9, P=0.004), 12 (beta=-3.4, P=0.001), and 24 months of age (beta=-3.2, P=0.001); TSH > 5 μIU/mL at any time after treatment initiation (beta=-3.6, P<0.001); and increase in LT4 dose by more than twice (beta=-3.2, P<0.001).</p><p><strong>Conclusion: </strong>Discrimination between PCH and TCH was achieved based on serum TSH concentrations at diagnosis, TSH > 5 μIU/mL during treatment, LT4 dose, LT4 > 50 µg during treatment, and increasing LT4 dose during treatment.</p>","PeriodicalId":44915,"journal":{"name":"Annals of Pediatric Endocrinology & Metabolism","volume":" ","pages":"149-156"},"PeriodicalIF":3.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235431/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pediatric Endocrinology & Metabolism","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.6065/apem.2448126.063","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To identify clinical predictors of permanent congenital hypothyroidism (PCH) and transient congenital hypothyroidism (TCH).
Methods: This retrospective cohort study enrolled neonates with risk factors for congenital hypothyroidism as diagnosed by neonatal screening test or blood testing. Levothyroxine (LT4) dose and serum thyroid stimulating hormone (TSH) concentrations were recorded from birth to 3 years of age.
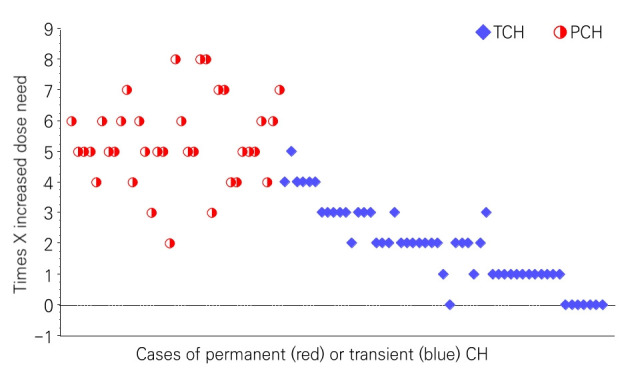
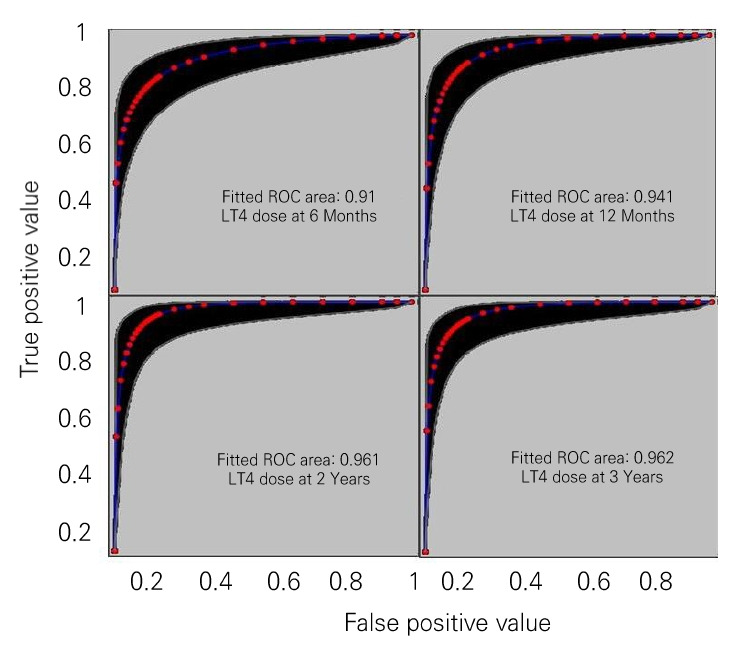
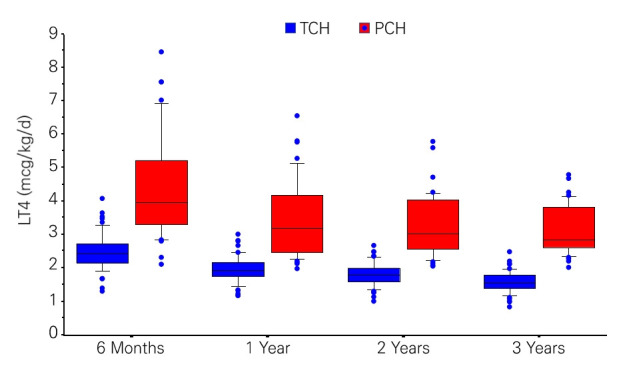
Results: We enrolled 88 neonates, 35 with PCH and 53 with TCH. An LT4 dose > 3.8 μg/kg/day at 6 months (sensitivity 62%, specificity 96%), 3.0 μg/kg/day at 12 months (64%, 97%, respectively), 2.6 μg/kg/day at 2 years (80%, 98%), and 2.5 μg/kg/day at 3 years (89%, 98%) of age could predict PCH. Daily total LT4 doses > 50 µg at any time during the follow-up period were found solely in the PCH group (28% vs 0%, P<0.001). Independent discriminative predictors of PCH and TCH were TSH concentrations at diagnosis (beta=-4.3, P<0.001); daily LT4 dose at 6 (beta=-2.9, P=0.004), 12 (beta=-3.4, P=0.001), and 24 months of age (beta=-3.2, P=0.001); TSH > 5 μIU/mL at any time after treatment initiation (beta=-3.6, P<0.001); and increase in LT4 dose by more than twice (beta=-3.2, P<0.001).
Conclusion: Discrimination between PCH and TCH was achieved based on serum TSH concentrations at diagnosis, TSH > 5 μIU/mL during treatment, LT4 dose, LT4 > 50 µg during treatment, and increasing LT4 dose during treatment.
期刊介绍:
The Annals of Pediatric Endocrinology & Metabolism Journal is the official publication of the Korean Society of Pediatric Endocrinology. Its formal abbreviated title is “Ann Pediatr Endocrinol Metab”. It is a peer-reviewed open access journal of medicine published in English. The journal was launched in 1996 under the title of ‘Journal of Korean Society of Pediatric Endocrinology’ until 2011 (pISSN 1226-2242). Since 2012, the title is now changed to ‘Annals of Pediatric Endocrinology & Metabolism’. The Journal is published four times per year on the last day of March, June, September, and December. It is widely distributed for free to members of the Korean Society of Pediatric Endocrinology, medical schools, libraries, and academic institutions. The journal is indexed/tracked/covered by web sites of PubMed Central, PubMed, Emerging Sources Citation Index (ESCI), Scopus, EBSCO, EMBASE, KoreaMed, KoMCI, KCI, Science Central, DOI/CrossRef, Directory of Open Access Journals(DOAJ), and Google Scholar. The aims of Annals of Pediatric Endocrinology & Metabolism are to contribute to the advancements in the fields of pediatric endocrinology & metabolism through the scientific reviews and interchange of all of pediatric endocrinology and metabolism. It aims to reflect the latest clinical, translational, and basic research trends from worldwide valuable achievements. In addition, genome research, epidemiology, public education and clinical practice guidelines in each country are welcomed for publication. The Journal particularly focuses on research conducted with Asian-Pacific children whose genetic and environmental backgrounds are different from those of the Western. Area of specific interest include the following : Growth, puberty, glucose metabolism including diabetes mellitus, obesity, nutrition, disorders of sexual development, pituitary, thyroid, parathyroid, adrenal cortex, bone or other endocrine and metabolic disorders from infancy through adolescence.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
