Allison Dorneo, Yanlei Ma, Melissa M Garrido, Steven D Pizer, Paul R Shafer, Thomas C Tsai, Austin B Frakt, Jose F Figueroa
{"title":"Characteristics and Benefit Design of Veteran Medicare Advantage Affinity Plans.","authors":"Allison Dorneo, Yanlei Ma, Melissa M Garrido, Steven D Pizer, Paul R Shafer, Thomas C Tsai, Austin B Frakt, Jose F Figueroa","doi":"10.1001/jamahealthforum.2025.0159","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Recently, there has been an emergence of veteran Medicare Advantage affinity plans (VMAPs) marketing to veterans, including those dually covered by the Veterans Health Administration (VHA). To date, limited evidence exists characterizing what benefits VMAPs offer and their veteran enrollees.</p><p><strong>Objective: </strong>To examine plan-level differences between VMAPs and other Medicare Advantage (MA) plans and characteristics of their veteran enrollees.</p><p><strong>Design, setting, and participants: </strong>This cross-sectional study compared the plan benefit design, supplemental benefit offerings, and veteran enrollee characteristics of all VMAP and other MA plan enrollees in 2022 using standardized mean differences (SMDs). VMAPs were identified based on military-associated words in their plan name and further validated through a web-based search. Data were analyzed from April 2023 to August 2024.</p><p><strong>Exposure: </strong>VMAP designation.</p><p><strong>Main outcomes and measures: </strong>Plan-level characteristics, supplemental benefits, and veteran enrollee characteristics.</p><p><strong>Results: </strong>The sample included 188 VMAPs with 179 449 veteran enrollees and 3442 other MA plans with 954 581 veteran enrollees. A total of 1 088 938 (96.0%) were male, 3558 (0.3%) were American Indian or Alaska Native, 8845 (0.8%) were Asian or Pacific Islander, 162 934 (14.4%) were Black, 61 264 (5.4%) were Hispanic, and 876 234 (77.3%) were White; the mean (SD) age was 75.9 (8.6) years. Most VMAPs were administered by for-profit insurers (173 [92.0%]; SMD, 0.42), including Aetna (46 [24.9%]), Humana (36 [19.5%]), and United HealthCare (49 [26.5%]). Compared with veterans in other MA plans, veterans in VMAPs were slightly younger (mean [SD] age, 73.7 [8.0] years vs 76.3 [8.7] years; SMD, 0.31), more likely to be Black (34 837 [19.4%] vs 128 097 [13.4%]; SMD, 0.18), and more likely to have zero cost sharing for VHA services (ie, priority group 1) (62 056 [34.6%] vs 195 688 [20.5%]; SMD, 0.40). VMAPs were more likely than other MA plans to offer $0 plan premiums (186 [98.9%] vs 2064 [60.0%]; SMD, 1.10), and Medicare Part B premium reductions (140 [74.5%] vs 298 [8.7%]; SMD, 1.80), averaging $33 more in cash back benefits. Only 1 VMAP offered Medicare Part D coverage compared with most other MA plans (1 [0.5%] vs 3293 [95.7%]; SMD, 6.23). VMAPs were more likely than other MA plans to provide comprehensive dental coverage (179 [95.2%] vs 3006 [87.3%]; SMD, 0.28), hearing aids (184 [97.9%] vs 3012 [87.5%]; SMD, 0.40), eyewear (188 [100%] vs 3620 [94.7%]; SMD, 0.33), over-the-counter drug coverage (179 [95.2%] vs 2831 [82.2%]; SMD, 0.42), and meal benefits (151 [80.3%] vs 2348 [68.2%]; SMD, 0.28).</p><p><strong>Conclusions and relevance: </strong>This study found that MA insurers-specifically VMAPs-engaged in targeted marketing to veterans, offering $0 premiums, cash back benefits, and supplemental benefits. However, nearly all VMAPs excluded Medicare Part D, likely designed to attract veteran enrollees who use VHA care, making them low-cost enrollees to the plan. Since the VHA cannot bill plans for Medicare-covered services, VMAPs may be increasing wasteful federal spending.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 3","pages":"e250159"},"PeriodicalIF":11.3000,"publicationDate":"2025-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11953753/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.0159","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Recently, there has been an emergence of veteran Medicare Advantage affinity plans (VMAPs) marketing to veterans, including those dually covered by the Veterans Health Administration (VHA). To date, limited evidence exists characterizing what benefits VMAPs offer and their veteran enrollees.
Objective: To examine plan-level differences between VMAPs and other Medicare Advantage (MA) plans and characteristics of their veteran enrollees.
Design, setting, and participants: This cross-sectional study compared the plan benefit design, supplemental benefit offerings, and veteran enrollee characteristics of all VMAP and other MA plan enrollees in 2022 using standardized mean differences (SMDs). VMAPs were identified based on military-associated words in their plan name and further validated through a web-based search. Data were analyzed from April 2023 to August 2024.
Exposure: VMAP designation.
Main outcomes and measures: Plan-level characteristics, supplemental benefits, and veteran enrollee characteristics.
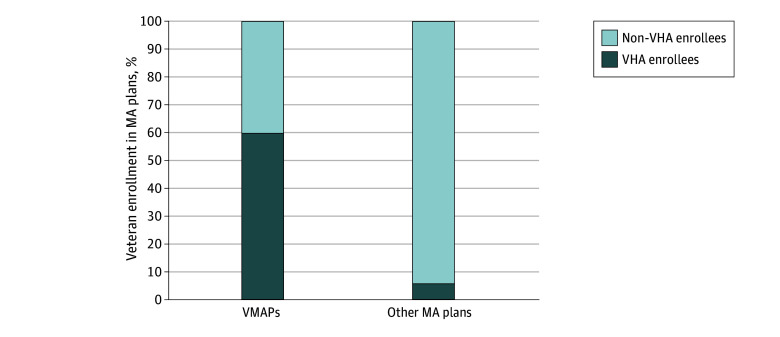
Results: The sample included 188 VMAPs with 179 449 veteran enrollees and 3442 other MA plans with 954 581 veteran enrollees. A total of 1 088 938 (96.0%) were male, 3558 (0.3%) were American Indian or Alaska Native, 8845 (0.8%) were Asian or Pacific Islander, 162 934 (14.4%) were Black, 61 264 (5.4%) were Hispanic, and 876 234 (77.3%) were White; the mean (SD) age was 75.9 (8.6) years. Most VMAPs were administered by for-profit insurers (173 [92.0%]; SMD, 0.42), including Aetna (46 [24.9%]), Humana (36 [19.5%]), and United HealthCare (49 [26.5%]). Compared with veterans in other MA plans, veterans in VMAPs were slightly younger (mean [SD] age, 73.7 [8.0] years vs 76.3 [8.7] years; SMD, 0.31), more likely to be Black (34 837 [19.4%] vs 128 097 [13.4%]; SMD, 0.18), and more likely to have zero cost sharing for VHA services (ie, priority group 1) (62 056 [34.6%] vs 195 688 [20.5%]; SMD, 0.40). VMAPs were more likely than other MA plans to offer $0 plan premiums (186 [98.9%] vs 2064 [60.0%]; SMD, 1.10), and Medicare Part B premium reductions (140 [74.5%] vs 298 [8.7%]; SMD, 1.80), averaging $33 more in cash back benefits. Only 1 VMAP offered Medicare Part D coverage compared with most other MA plans (1 [0.5%] vs 3293 [95.7%]; SMD, 6.23). VMAPs were more likely than other MA plans to provide comprehensive dental coverage (179 [95.2%] vs 3006 [87.3%]; SMD, 0.28), hearing aids (184 [97.9%] vs 3012 [87.5%]; SMD, 0.40), eyewear (188 [100%] vs 3620 [94.7%]; SMD, 0.33), over-the-counter drug coverage (179 [95.2%] vs 2831 [82.2%]; SMD, 0.42), and meal benefits (151 [80.3%] vs 2348 [68.2%]; SMD, 0.28).
Conclusions and relevance: This study found that MA insurers-specifically VMAPs-engaged in targeted marketing to veterans, offering $0 premiums, cash back benefits, and supplemental benefits. However, nearly all VMAPs excluded Medicare Part D, likely designed to attract veteran enrollees who use VHA care, making them low-cost enrollees to the plan. Since the VHA cannot bill plans for Medicare-covered services, VMAPs may be increasing wasteful federal spending.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
