Frederike Bieling, Robert A Cesnjevar, Michela Cuomo, Annika Weigelt, Sven Dittrich, Ariawan Purbojo
{"title":"Anatomical Left Superior Vena Cava Correction: An Option for Left Ventricular Recruitment?","authors":"Frederike Bieling, Robert A Cesnjevar, Michela Cuomo, Annika Weigelt, Sven Dittrich, Ariawan Purbojo","doi":"10.1055/a-2531-3126","DOIUrl":null,"url":null,"abstract":"<p><p>Left superior vena cava (LSVC)-related obstruction of mitral inflow is a rare condition in patients with complex cardiac anomalies like hypoplastic left heart complex. We report on the impact of establishing LSVC to right superior vena cava (RSVC) continuity on the growth of borderline hypoplastic left ventricular structures as an addendum to our previously published work.Twenty-two patients underwent LSVC to RSVC anastomosis, whereas six had LSVC ligation (<i>n</i> = 4) or clip closure (<i>n</i> = 2), all alongside congenital heart defect correction. The indication was LSVC-related obstruction of left ventricular inflow due to a dilated coronary sinus. Clinical data were systematically reviewed, with regular follow-up. Left ventricular end diastolic diameters (LVEDD), aortic valve diameters, and left ventricular outflow tract (LVOT) diameters were recorded using echocardiography.Follow-up showed 90% survival at 3.3 ± 0.4 years. Mean LVEDD Z-scores improved from -2.19 ± 0.35 to -1.24 ± 0.26 after repair (<i>p</i> < 0.01) and to -1.33 ± 0.56 at 6-month follow-up. In patients without mitral repair, LVEDD Z-scores improved from -2.11 ± 0.62 preoperatively to -1.85 ± 0.88 postoperatively (<i>p</i> < 0.05). LVOT Z-scores increased from -2.49 ± 0.48 to -0.87 ± 0.75 (<i>p</i> < 0.05) and aortic valve Z-scores improved from -1.08 ± 0.57 to 0.5 ± 0.39 over 24 months (<i>p</i> < 0.05).Anatomical LSVC correction may improve left ventricular filling and growth of the left ventricle, aortic valve, and LVOT in patients with borderline left ventricles and could be considered without as a potential recruitment strategy.</p>","PeriodicalId":23057,"journal":{"name":"Thoracic and Cardiovascular Surgeon","volume":"73 S 03","pages":"e21-e30"},"PeriodicalIF":1.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11970464/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic and Cardiovascular Surgeon","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2531-3126","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
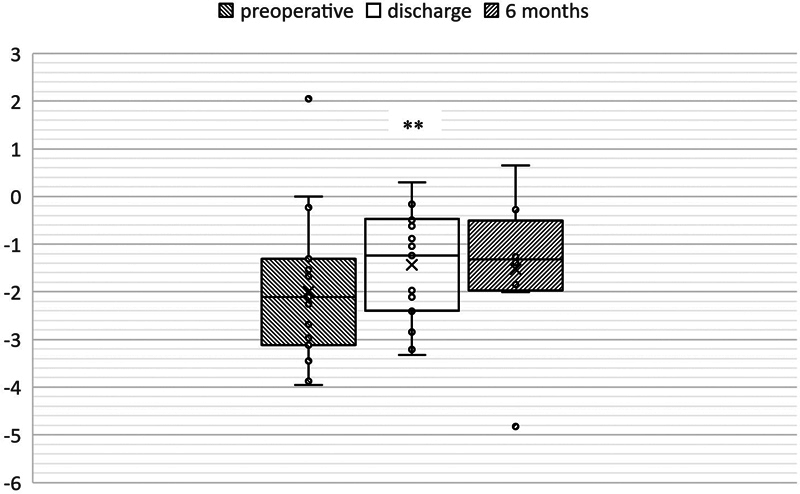
Left superior vena cava (LSVC)-related obstruction of mitral inflow is a rare condition in patients with complex cardiac anomalies like hypoplastic left heart complex. We report on the impact of establishing LSVC to right superior vena cava (RSVC) continuity on the growth of borderline hypoplastic left ventricular structures as an addendum to our previously published work.Twenty-two patients underwent LSVC to RSVC anastomosis, whereas six had LSVC ligation (n = 4) or clip closure (n = 2), all alongside congenital heart defect correction. The indication was LSVC-related obstruction of left ventricular inflow due to a dilated coronary sinus. Clinical data were systematically reviewed, with regular follow-up. Left ventricular end diastolic diameters (LVEDD), aortic valve diameters, and left ventricular outflow tract (LVOT) diameters were recorded using echocardiography.Follow-up showed 90% survival at 3.3 ± 0.4 years. Mean LVEDD Z-scores improved from -2.19 ± 0.35 to -1.24 ± 0.26 after repair (p < 0.01) and to -1.33 ± 0.56 at 6-month follow-up. In patients without mitral repair, LVEDD Z-scores improved from -2.11 ± 0.62 preoperatively to -1.85 ± 0.88 postoperatively (p < 0.05). LVOT Z-scores increased from -2.49 ± 0.48 to -0.87 ± 0.75 (p < 0.05) and aortic valve Z-scores improved from -1.08 ± 0.57 to 0.5 ± 0.39 over 24 months (p < 0.05).Anatomical LSVC correction may improve left ventricular filling and growth of the left ventricle, aortic valve, and LVOT in patients with borderline left ventricles and could be considered without as a potential recruitment strategy.
左上腔静脉(LSVC)相关二尖瓣流入阻塞在左心发育不全等复杂心脏异常患者中是一种罕见的情况。我们报告建立LSVC至右上腔静脉(RSVC)连续性对边缘性左室发育不全结构生长的影响,作为我们先前发表的工作的补充。22例患者行LSVC与RSVC吻合,而6例患者行LSVC结扎(n = 4)或夹子闭合(n = 2),均伴先天性心脏缺损矫正。适应症是由冠状动脉窦扩张引起的左室血流梗阻。系统回顾临床资料,定期随访。超声心动图记录左室舒张末期直径(LVEDD)、主动脉瓣直径和左室流出道直径(LVOT)。随访显示,3.3±0.4年生存率为90%。修复后平均LVEDD z -评分由-2.19±0.35分改善至-1.24±0.26分(p p p p
期刊介绍:
The Thoracic and Cardiovascular Surgeon publishes articles of the highest standard from internationally recognized thoracic and cardiovascular surgeons, cardiologists, anesthesiologists, physiologists, and pathologists. This journal is an essential resource for anyone working in this field.
Original articles, short communications, reviews and important meeting announcements keep you abreast of key clinical advances, as well as providing the theoretical background of cardiovascular and thoracic surgery. Case reports are published in our Open Access companion journal The Thoracic and Cardiovascular Surgeon Reports.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
