Benefits, burden, and harms of computer aided polyp detection with artificial intelligence in colorectal cancer screening: microsimulation modelling study.
Natalie Halvorsen, Cesare Hassan, Loredana Correale, Nastazja Pilonis, Lise M Helsingen, Marco Spadaccini, Alessandro Repici, Farid Foroutan, Per Olav Vandvik, Shanaz Sultan, Magnus Løberg, Mette Kalager, Yuichi Mori, Michael Bretthauer
{"title":"Benefits, burden, and harms of computer aided polyp detection with artificial intelligence in colorectal cancer screening: microsimulation modelling study.","authors":"Natalie Halvorsen, Cesare Hassan, Loredana Correale, Nastazja Pilonis, Lise M Helsingen, Marco Spadaccini, Alessandro Repici, Farid Foroutan, Per Olav Vandvik, Shanaz Sultan, Magnus Løberg, Mette Kalager, Yuichi Mori, Michael Bretthauer","doi":"10.1136/bmjmed-2025-001446","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong></p><p><strong>Objective: </strong>To estimate the benefits, burden, and harms of implementing computer aided detection (CADe) of polyps in colonoscopy of population based screening programmes for colorectal cancer.</p><p><strong>Design: </strong>Microsimulation modelling study.</p><p><strong>Setting: </strong>Cost effectiveness working package in the OperA (optimising colorectal cancer prevention through personalised treatment with artificial intelligence) project. A parallel guideline committee panel (BMJ Rapid recommendation) was consulted in defining the screening interventions and selection of outcome measures.</p><p><strong>Population: </strong>Four cohorts of 100 000 European individuals aged 60-69 years.</p><p><strong>Intervention: </strong>The intervention was one screening of colonoscopy and a screening of colonoscopy after faecal immunochemical test every other year with CADe. The comparison group had the same screening every other year without CADe.</p><p><strong>Main outcome measures: </strong>Benefits (colorectal cancer incidence and death), burden (surveillance colonoscopies), and harms (colonoscopy related adverse events) over 10 years were measured. The certainty in each outcome was assessed by use of the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach.</p><p><strong>Results: </strong>For 100 000 individuals participating in colonoscopy screening, 824 (0.82%) were diagnosed with colorectal cancer within 10 years without CADe versus 713 (0.71%) with CADe (risk difference -0.11% (95% CI -0.43% to 0.21%)). For faecal immunochemical test screening colonoscopy, the risk was 5.82% (n=5820) without CADe versus 5.77% (n=5770) with CADe (difference -0.05% (-0.33% to 0.15%)). The risk of surveillance colonoscopy increased from 26.45% (n=26 453) to 32.82% (n=32 819) (difference 6.37% (5.8% to 6.9%)) for colonoscopy screening and from 52.26% (n=52 263) to 53.08% (n=53 082) (difference 0.82% (0.38% to 1.26%)) for faecal immunochemical test screening colonoscopy. No significant differences were noted in adverse events related to the colonoscopy between CADe and no CADe. The model estimates were sensitive to the assumed effects of screening on colorectal cancer risk and of CADe on adenoma detection rates. All outcomes were graded as low certainty.</p><p><strong>Conclusion: </strong>With low certainty of evidence, adoption of CADe in population based screening provides small and uncertain clinical meaningful benefit, no incremental harms, and increased surveillance burden after screening.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"4 1","pages":"e001446"},"PeriodicalIF":10.0000,"publicationDate":"2025-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11955961/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2025-001446","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Abstract:
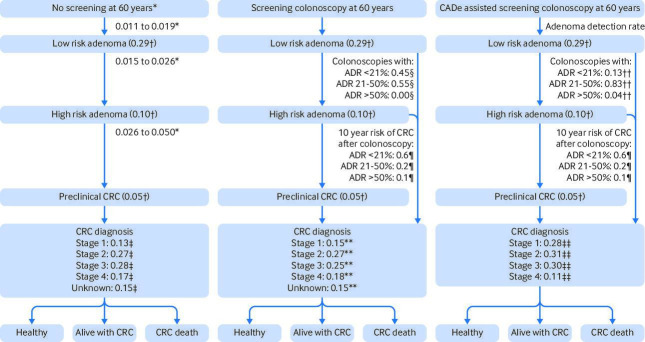
Objective: To estimate the benefits, burden, and harms of implementing computer aided detection (CADe) of polyps in colonoscopy of population based screening programmes for colorectal cancer.
Design: Microsimulation modelling study.
Setting: Cost effectiveness working package in the OperA (optimising colorectal cancer prevention through personalised treatment with artificial intelligence) project. A parallel guideline committee panel (BMJ Rapid recommendation) was consulted in defining the screening interventions and selection of outcome measures.
Population: Four cohorts of 100 000 European individuals aged 60-69 years.
Intervention: The intervention was one screening of colonoscopy and a screening of colonoscopy after faecal immunochemical test every other year with CADe. The comparison group had the same screening every other year without CADe.
Main outcome measures: Benefits (colorectal cancer incidence and death), burden (surveillance colonoscopies), and harms (colonoscopy related adverse events) over 10 years were measured. The certainty in each outcome was assessed by use of the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach.
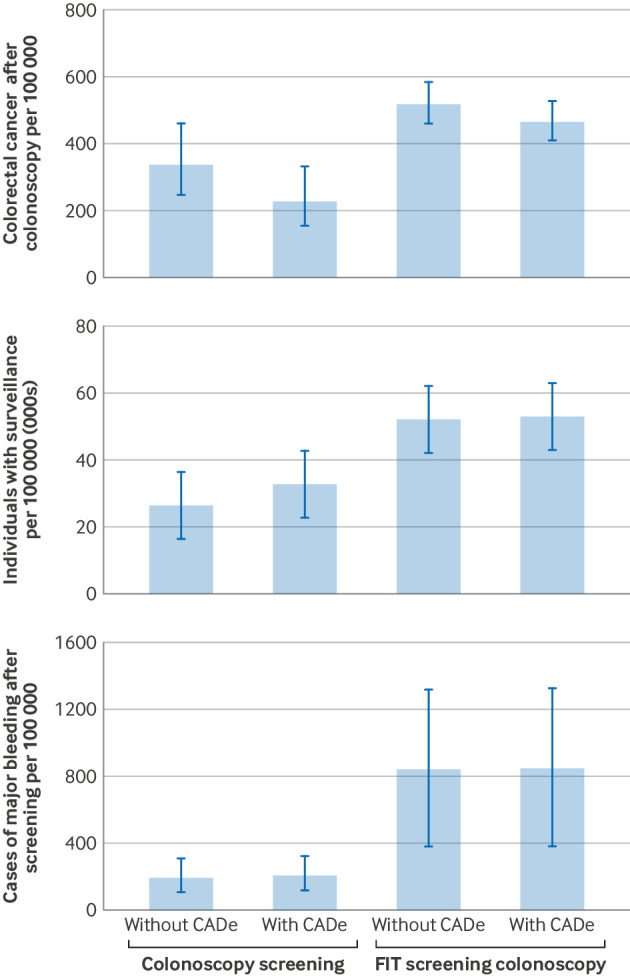
Results: For 100 000 individuals participating in colonoscopy screening, 824 (0.82%) were diagnosed with colorectal cancer within 10 years without CADe versus 713 (0.71%) with CADe (risk difference -0.11% (95% CI -0.43% to 0.21%)). For faecal immunochemical test screening colonoscopy, the risk was 5.82% (n=5820) without CADe versus 5.77% (n=5770) with CADe (difference -0.05% (-0.33% to 0.15%)). The risk of surveillance colonoscopy increased from 26.45% (n=26 453) to 32.82% (n=32 819) (difference 6.37% (5.8% to 6.9%)) for colonoscopy screening and from 52.26% (n=52 263) to 53.08% (n=53 082) (difference 0.82% (0.38% to 1.26%)) for faecal immunochemical test screening colonoscopy. No significant differences were noted in adverse events related to the colonoscopy between CADe and no CADe. The model estimates were sensitive to the assumed effects of screening on colorectal cancer risk and of CADe on adenoma detection rates. All outcomes were graded as low certainty.
Conclusion: With low certainty of evidence, adoption of CADe in population based screening provides small and uncertain clinical meaningful benefit, no incremental harms, and increased surveillance burden after screening.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
