Sayo Masuko, Yusuke Matsuyama, Shiho Kino, Katsunori Kondo, Jun Aida
{"title":"Reply to: Comment on: Changes in Leisure Activity, All-Cause Mortality, and Functional Disability in Older Japanese Adults","authors":"Sayo Masuko, Yusuke Matsuyama, Shiho Kino, Katsunori Kondo, Jun Aida","doi":"10.1111/jgs.19453","DOIUrl":null,"url":null,"abstract":"<p>We appreciate Dr. Kars and colleagues for their interest in our study [<span>1</span>] examining the association between changes in the presence of leisure activities from 2010 to 2013 and their impact on the occurrence of all-cause mortality and functional disability until 2020 among older Japanese adults. We are grateful for the opportunity to reply to their letter to the Editor [<span>2</span>].</p><p>In this letter, they highlight an important point regarding our study. We agree with their critical opinion that cognitive complaints and depression in 2013 must be considered new confounders, as they can be a cause of discontinuation of leisure activities.</p><p>Cognitive complaints and depression are strongly associated with physical activity levels. Leisure activities include many physical activities such as running, golf, and dancing [<span>3</span>]. Consequently, it is possible that those who engaged in physical leisure activities in 2010 discontinued participation in such activity in 2013 because of worsening cognitive function and depression from 2010 to 2013. Therefore, adjusting for cognitive complaints and depression in 2013 as covariates, in addition to existing covariates (depression, cognitive complaints, instrumental activities of daily living [IADL], self-rated health, sex, age, education, equivalent income, employment status, longest occupation, living alone, marital status, smoking, alcohol, and body mass index [BMI] in 2010, and changes in five major comorbidities [cancer, heart disease, stroke, diabetes, and respiratory disease] and other comorbidities from 2010 to 2013), is important to improve on previous findings.</p><p>Therefore, we repeated the analysis with the covariates of changes in cognitive complaints and depression from 2010 to 2013 rather than cognitive complaints and depression in 2010. In our previous analyses, depression was assessed using three categories: none/mild (Geriatric Depression Scale [GDS] < 5), moderate (5 ≤ GDS < 10), and severe (GDS ≥ 10) [<span>4</span>]. In this additional analysis, depression was first assessed as a binary variable in 2010 and 2013; none/mild (GDS < 5), moderate or severe (GDS ≥ 5) [<span>5</span>], and changes from 2010 to 2013 were assessed using four categories. This four-category categorization was the same as that of the covariates for changes in the presence of comorbidities. Changes in cognitive complaints were assessed using the same four categories.</p><p>The results of this analysis are shown in Figure 1. Among those who were engaged in leisure activities in 2010 but discontinued participation in 2013 (Presence 10–No presence 13), the hazard ratios for mortality and functional disability were 1.03 (95% confidence interval [95% CI], 0.84–1.26) and 1.38 (95% CI, 1.08–1.76), respectively, compared with those of participants without leisure activities in both 2010 and 2013. Also, among those who were not engaged in leisure activities in 2010 but began participating in leisure activities in 2013 (No presence 10–Presence 13), the hazard ratios for mortality and functional disability were 0.83 (95% CI, 0.75–0.91) and 0.91 (95% CI, 0.81–1.04), respectively. These results are similar to those of previous studies that only adjusted for cognitive complaints and depression in 2010 [<span>1</span>].</p><p>In conclusion, the additional analysis suggested by Dr. Kars and colleagues confirmed that the risk of mortality was reduced even when participation in leisure activities was initiated after baseline, and the risk of functional disability increased when leisure activities were discontinued after baseline.</p><p>S.M. and J.A. performed the analysis and wrote the reply; the other authors critically revised the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for any part of this work.</p><p>The authors declare no conflicts of interest.</p><p>This publication is linked to a related article by Yilmaz Kars et al. To view this article, visit https://doi.org/10.1111/jgs.19451.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"73 7","pages":"2296-2297"},"PeriodicalIF":4.5000,"publicationDate":"2025-04-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19453","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19453","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
We appreciate Dr. Kars and colleagues for their interest in our study [1] examining the association between changes in the presence of leisure activities from 2010 to 2013 and their impact on the occurrence of all-cause mortality and functional disability until 2020 among older Japanese adults. We are grateful for the opportunity to reply to their letter to the Editor [2].
In this letter, they highlight an important point regarding our study. We agree with their critical opinion that cognitive complaints and depression in 2013 must be considered new confounders, as they can be a cause of discontinuation of leisure activities.
Cognitive complaints and depression are strongly associated with physical activity levels. Leisure activities include many physical activities such as running, golf, and dancing [3]. Consequently, it is possible that those who engaged in physical leisure activities in 2010 discontinued participation in such activity in 2013 because of worsening cognitive function and depression from 2010 to 2013. Therefore, adjusting for cognitive complaints and depression in 2013 as covariates, in addition to existing covariates (depression, cognitive complaints, instrumental activities of daily living [IADL], self-rated health, sex, age, education, equivalent income, employment status, longest occupation, living alone, marital status, smoking, alcohol, and body mass index [BMI] in 2010, and changes in five major comorbidities [cancer, heart disease, stroke, diabetes, and respiratory disease] and other comorbidities from 2010 to 2013), is important to improve on previous findings.
Therefore, we repeated the analysis with the covariates of changes in cognitive complaints and depression from 2010 to 2013 rather than cognitive complaints and depression in 2010. In our previous analyses, depression was assessed using three categories: none/mild (Geriatric Depression Scale [GDS] < 5), moderate (5 ≤ GDS < 10), and severe (GDS ≥ 10) [4]. In this additional analysis, depression was first assessed as a binary variable in 2010 and 2013; none/mild (GDS < 5), moderate or severe (GDS ≥ 5) [5], and changes from 2010 to 2013 were assessed using four categories. This four-category categorization was the same as that of the covariates for changes in the presence of comorbidities. Changes in cognitive complaints were assessed using the same four categories.
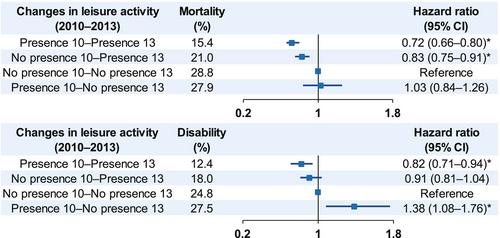
The results of this analysis are shown in Figure 1. Among those who were engaged in leisure activities in 2010 but discontinued participation in 2013 (Presence 10–No presence 13), the hazard ratios for mortality and functional disability were 1.03 (95% confidence interval [95% CI], 0.84–1.26) and 1.38 (95% CI, 1.08–1.76), respectively, compared with those of participants without leisure activities in both 2010 and 2013. Also, among those who were not engaged in leisure activities in 2010 but began participating in leisure activities in 2013 (No presence 10–Presence 13), the hazard ratios for mortality and functional disability were 0.83 (95% CI, 0.75–0.91) and 0.91 (95% CI, 0.81–1.04), respectively. These results are similar to those of previous studies that only adjusted for cognitive complaints and depression in 2010 [1].
In conclusion, the additional analysis suggested by Dr. Kars and colleagues confirmed that the risk of mortality was reduced even when participation in leisure activities was initiated after baseline, and the risk of functional disability increased when leisure activities were discontinued after baseline.
S.M. and J.A. performed the analysis and wrote the reply; the other authors critically revised the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for any part of this work.
The authors declare no conflicts of interest.
This publication is linked to a related article by Yilmaz Kars et al. To view this article, visit https://doi.org/10.1111/jgs.19451.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.





 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
