Maria Teresa Bruno, Nazario Cassaro, Francesca Bica, Sara Boemi
{"title":"Progression of CIN1/LSIL HPV Persistent of the Cervix: Actual Progression or CIN3 Coexistence.","authors":"Maria Teresa Bruno, Nazario Cassaro, Francesca Bica, Sara Boemi","doi":"10.1155/2021/6627531","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The natural history of the CIN1 lesions is characterized by an elevated rate of spontaneous regression (80%), some authors recognize a capacity to progress to HSIL in 10% of cases, and other authors do not recognize the capacity of progression of LSIL (CIN1). This study was aimed to evaluate the incidence of progression to HSIL (CIN3) in women with a histological diagnosis of LSIL (CIN1). Furthermore, to this end, we studied the histological outcomes of cone specimens collected by the LEEP.</p><p><strong>Methods: </strong>All the data were retrospectively analyzed. All participants underwent a follow-up of 4 years, during which each woman underwent an HPV test and genotyping, cervical cytological sampling, or biopsy every six months. The endpoint was the histological confirmation of CIN3 lesions in any moment during follow-up.</p><p><strong>Results: </strong>Progression to CIN3 occurred in 7 cases (1,5%). Analyzing the histological exams of the cones of the 7 cases that progressed to CIN3, we found the coexistence of CIN1 and CIN3 lesions in all cases.</p><p><strong>Conclusion: </strong>After 4 years of follow-up, only 1.5% (7/475) of the women with LSIL developed CIN3, all within the first two years of follow-up, and were immediately treated. The most likely explanations for \"progression\" from LSIL to HSIL are (1) actual progression, (2) underdiagnosis of HSIL on initial biopsy, (3) overdiagnosis of HSIL on follow-up biopsy/cone, and (4) CIN3 arose de novo. Analyzing the histological exams of the cones of the 7 cases that progressed to high-grade, we found the coexistence of CIN1 and CIN3 lesions in all cases. Some recent studies have shown that a viral genotype corresponds to different lesions in the same cervix; therefore, CIN1 coexisting with CIN3 does not always indicate progression of CIN1. Other authors have doubted the capacity of LSIL to progress.</p>","PeriodicalId":13546,"journal":{"name":"Infectious Diseases in Obstetrics and Gynecology","volume":"2021 ","pages":"6627531"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7972837/pdf/","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/6627531","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 11
Abstract
Objective: The natural history of the CIN1 lesions is characterized by an elevated rate of spontaneous regression (80%), some authors recognize a capacity to progress to HSIL in 10% of cases, and other authors do not recognize the capacity of progression of LSIL (CIN1). This study was aimed to evaluate the incidence of progression to HSIL (CIN3) in women with a histological diagnosis of LSIL (CIN1). Furthermore, to this end, we studied the histological outcomes of cone specimens collected by the LEEP.
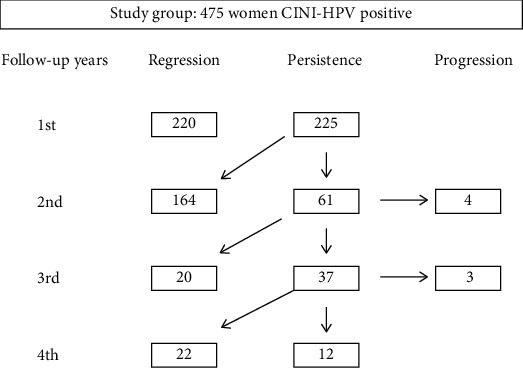
Methods: All the data were retrospectively analyzed. All participants underwent a follow-up of 4 years, during which each woman underwent an HPV test and genotyping, cervical cytological sampling, or biopsy every six months. The endpoint was the histological confirmation of CIN3 lesions in any moment during follow-up.
Results: Progression to CIN3 occurred in 7 cases (1,5%). Analyzing the histological exams of the cones of the 7 cases that progressed to CIN3, we found the coexistence of CIN1 and CIN3 lesions in all cases.
Conclusion: After 4 years of follow-up, only 1.5% (7/475) of the women with LSIL developed CIN3, all within the first two years of follow-up, and were immediately treated. The most likely explanations for "progression" from LSIL to HSIL are (1) actual progression, (2) underdiagnosis of HSIL on initial biopsy, (3) overdiagnosis of HSIL on follow-up biopsy/cone, and (4) CIN3 arose de novo. Analyzing the histological exams of the cones of the 7 cases that progressed to high-grade, we found the coexistence of CIN1 and CIN3 lesions in all cases. Some recent studies have shown that a viral genotype corresponds to different lesions in the same cervix; therefore, CIN1 coexisting with CIN3 does not always indicate progression of CIN1. Other authors have doubted the capacity of LSIL to progress.
期刊介绍:
Infectious Diseases in Obstetrics and Gynecology aims to disseminate new and important information to clinicians and other health care providers, scientists, and researchers involved in the study or treatment of infectious diseases, especially those affecting the female patient. Its ultimate aim is to advance knowledge and encourage research, thereby improving the prevention or diagnosis and treatment of patients affected by such diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
