Michael L Williams, Mathew P Doyle, Nicholas McNamara, Daniel Tardo, Manish Mathew, Benjamin Robinson
{"title":"Epidemiology of infective endocarditis before <i>versus</i> after change of international guidelines: a systematic review.","authors":"Michael L Williams, Mathew P Doyle, Nicholas McNamara, Daniel Tardo, Manish Mathew, Benjamin Robinson","doi":"10.1177/17539447211002687","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>All major international guidelines for the management of infective endocarditis (IE) have undergone major revisions, recommending antibiotic prophylaxis (AP) restriction to high-risk patients or foregoing AP completely. We performed a systematic review to investigate the effect of these guideline changes on the global incidence of IE.</p><p><strong>Methods: </strong>Electronic database searches were performed using Ovid Medline, EMBASE and Web of Science. Studies were included if they compared the incidence of IE prior to and following any change in international guideline recommendations. Relevant studies fulfilling the predefined search criteria were categorized according to their inclusion of either adult or pediatric patients. Incidence of IE, causative microorganisms and AP prescription rates were compared following international guideline updates.</p><p><strong>Results: </strong>Sixteen studies were included, reporting over 1.3 million cases of IE. The crude incidence of IE following guideline updates has increased globally. Adjusted incidence increased in one study after European guideline updates, while North American rates did not increase. Cases of IE with a causative pathogen identified ranged from 62% to 91%. Rates of streptococcal IE varied across adult and pediatric populations, while the relative proportion of staphylococcal IE increased (range pre-guidelines 16-24.8%, range post-guidelines 26-43%). AP prescription trends were reduced in both moderate and high-risk patients following guideline updates.</p><p><strong>Discussion: </strong>The restriction of AP to only high-risk patients has not resulted in an increase in the incidence of streptococcal IE in North American populations. The evidence of the impact of AP restriction on IE incidence is still unclear for other populations. Future population-based studies with adjusted incidence of IE, AP prescription rates and accurate pathogen identification are required to delineate findings further in these other regions.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"15 ","pages":"17539447211002687"},"PeriodicalIF":2.2000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/17539447211002687","citationCount":"20","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17539447211002687","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 20
Abstract
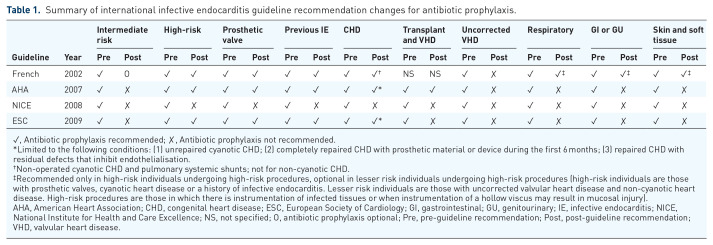
Introduction: All major international guidelines for the management of infective endocarditis (IE) have undergone major revisions, recommending antibiotic prophylaxis (AP) restriction to high-risk patients or foregoing AP completely. We performed a systematic review to investigate the effect of these guideline changes on the global incidence of IE.
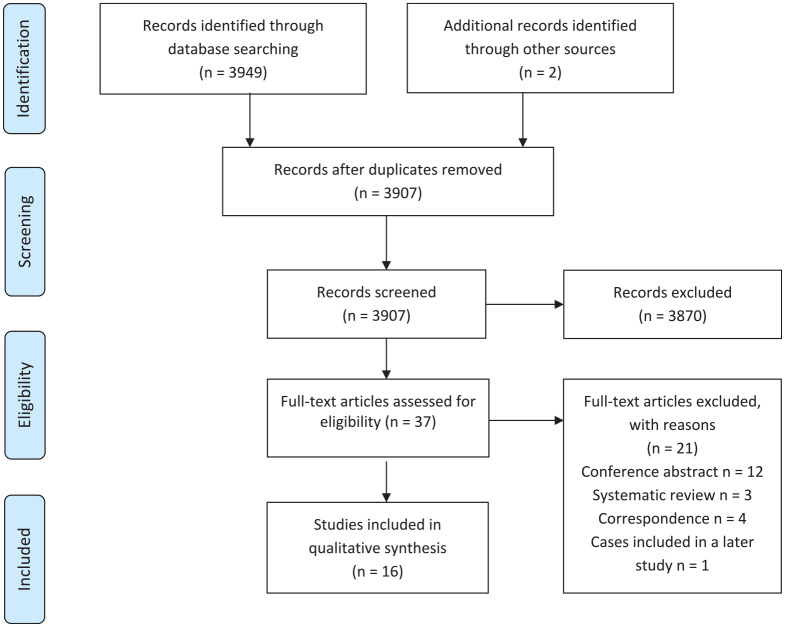
Methods: Electronic database searches were performed using Ovid Medline, EMBASE and Web of Science. Studies were included if they compared the incidence of IE prior to and following any change in international guideline recommendations. Relevant studies fulfilling the predefined search criteria were categorized according to their inclusion of either adult or pediatric patients. Incidence of IE, causative microorganisms and AP prescription rates were compared following international guideline updates.
Results: Sixteen studies were included, reporting over 1.3 million cases of IE. The crude incidence of IE following guideline updates has increased globally. Adjusted incidence increased in one study after European guideline updates, while North American rates did not increase. Cases of IE with a causative pathogen identified ranged from 62% to 91%. Rates of streptococcal IE varied across adult and pediatric populations, while the relative proportion of staphylococcal IE increased (range pre-guidelines 16-24.8%, range post-guidelines 26-43%). AP prescription trends were reduced in both moderate and high-risk patients following guideline updates.
Discussion: The restriction of AP to only high-risk patients has not resulted in an increase in the incidence of streptococcal IE in North American populations. The evidence of the impact of AP restriction on IE incidence is still unclear for other populations. Future population-based studies with adjusted incidence of IE, AP prescription rates and accurate pathogen identification are required to delineate findings further in these other regions.
导论:感染性心内膜炎(IE)管理的所有主要国际指南都经历了重大修订,建议对高危患者限制抗生素预防(AP)或完全放弃抗生素预防。我们进行了一项系统综述,以调查这些指南变化对IE全球发病率的影响。方法:采用Ovid Medline、EMBASE和Web of Science进行电子数据库检索。如果研究在国际指南建议改变之前和之后比较IE的发生率,则纳入研究。满足预定义检索标准的相关研究根据其包含的成人或儿童患者进行分类。在国际指南更新后,比较IE的发病率、致病微生物和AP处方率。结果:纳入了16项研究,报告了130多万例IE病例。指南更新后IE的粗发生率在全球范围内有所增加。在欧洲指南更新后,一项研究中调整后的发病率增加,而北美的发病率没有增加。具有病原鉴定的IE病例从62%到91%不等。成人和儿童人群中链球菌感染IE的比例各不相同,而葡萄球菌感染IE的相对比例有所增加(指南前范围16-24.8%,指南后范围26-43%)。指南更新后,中高危患者的AP处方趋势均有所减少。讨论:仅限高危患者使用AP并未导致北美人群链球菌IE发病率的增加。限制AP对其他人群IE发病率影响的证据尚不清楚。未来的基于人群的研究需要调整IE发病率,AP处方率和准确的病原体鉴定,以进一步描述这些地区的发现。
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
