Blaise Genton, Ivo Mueller, Inoni Betuela, Gerard Casey, Meza Ginny, Michael P Alpers, John C Reeder
{"title":"Rifampicin/Cotrimoxazole/Isoniazid versus mefloquine or quinine + sulfadoxine- pyrimethamine for malaria: a randomized trial.","authors":"Blaise Genton, Ivo Mueller, Inoni Betuela, Gerard Casey, Meza Ginny, Michael P Alpers, John C Reeder","doi":"10.1371/journal.pctr.0010038","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Previous studies of a fixed combination including cotrimoxazole, rifampicin, and isoniazid (Cotrifazid) showed efficacy against resistant strains of Plasmodium falciparum in animal models and in small-scale human studies. We conducted a multicentric noninferiority trial to assess the safety and efficacy of Cotrifazid against drug-resistant malaria in Papua New Guinea.</p><p><strong>Design: </strong>The trial design was open-label, block-randomised, comparative, and multicentric.</p><p><strong>Setting: </strong>The trial was conducted in four primary care health facilities, two in urban and two in rural areas of Madang and East Sepik Province, Papua New Guinea.</p><p><strong>Participants: </strong>Patients of all ages with recurrent uncomplicated malaria were included.</p><p><strong>Interventions: </strong>Patients were randomly assigned to receive Cotrifazid, mefloquine, or the standard treatment of quinine with sulfadoxine-pyrimethamine (SP).</p><p><strong>Outcome measures: </strong>Incidence of clinical and laboratory adverse events and rate of clinical and/or parasitological failure at day 14 were recorded.</p><p><strong>Results: </strong>The safety analysis population included 123 patients assigned to Cotrifazid, 123 to mefloquine, and 123 to quinine + SP. The Cotrifazid group experienced lower overall incidence of adverse events than the other groups. Among the efficacy analysis population (72 Cotrifazid, 71 mefloquine, and 75 quinine + SP), clinical failure rate (symptoms and parasite load) on day 14 was equivalent for the three groups (0% for Cotrifazid and mefloquine; 1% for quinine + SP), but parasitological failure rate (P. falciparum asexual blood-stage) was higher for Cotrifazid than for mefloquine or quinine + SP (9% [PCR corrected 8%] versus 0% and 3%, respectively [p = 0.02]).</p><p><strong>Conclusion: </strong>Despite what appears to be short-term clinical equivalence, the notable parasitological failure at day 14 in both P. falciparum and P. vivax makes Cotrifazid in its current formulation and regimen a poor alternative combination therapy for malaria.</p>","PeriodicalId":87416,"journal":{"name":"PLoS clinical trials","volume":"1 8","pages":"e38"},"PeriodicalIF":0.0000,"publicationDate":"2006-12-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1371/journal.pctr.0010038","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS clinical trials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pctr.0010038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
Abstract
Objectives: Previous studies of a fixed combination including cotrimoxazole, rifampicin, and isoniazid (Cotrifazid) showed efficacy against resistant strains of Plasmodium falciparum in animal models and in small-scale human studies. We conducted a multicentric noninferiority trial to assess the safety and efficacy of Cotrifazid against drug-resistant malaria in Papua New Guinea.
Design: The trial design was open-label, block-randomised, comparative, and multicentric.
Setting: The trial was conducted in four primary care health facilities, two in urban and two in rural areas of Madang and East Sepik Province, Papua New Guinea.
Participants: Patients of all ages with recurrent uncomplicated malaria were included.
Interventions: Patients were randomly assigned to receive Cotrifazid, mefloquine, or the standard treatment of quinine with sulfadoxine-pyrimethamine (SP).
Outcome measures: Incidence of clinical and laboratory adverse events and rate of clinical and/or parasitological failure at day 14 were recorded.
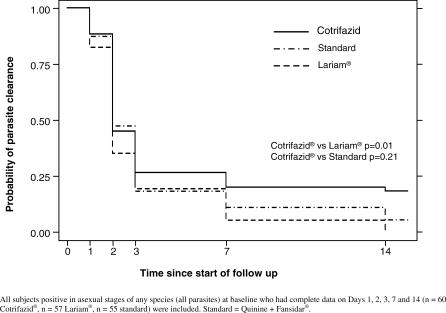
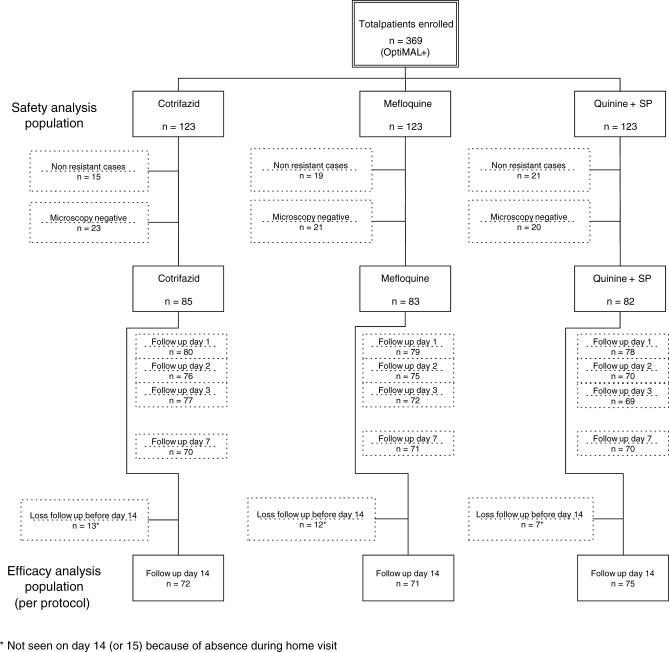
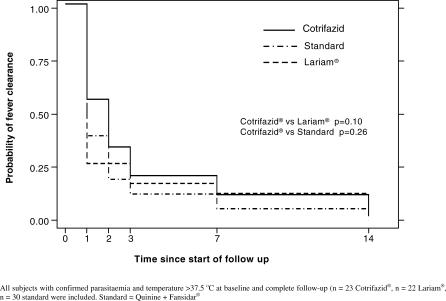
Results: The safety analysis population included 123 patients assigned to Cotrifazid, 123 to mefloquine, and 123 to quinine + SP. The Cotrifazid group experienced lower overall incidence of adverse events than the other groups. Among the efficacy analysis population (72 Cotrifazid, 71 mefloquine, and 75 quinine + SP), clinical failure rate (symptoms and parasite load) on day 14 was equivalent for the three groups (0% for Cotrifazid and mefloquine; 1% for quinine + SP), but parasitological failure rate (P. falciparum asexual blood-stage) was higher for Cotrifazid than for mefloquine or quinine + SP (9% [PCR corrected 8%] versus 0% and 3%, respectively [p = 0.02]).
Conclusion: Despite what appears to be short-term clinical equivalence, the notable parasitological failure at day 14 in both P. falciparum and P. vivax makes Cotrifazid in its current formulation and regimen a poor alternative combination therapy for malaria.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
