Stephanie T. Page, Thomas F. Kalhorn, William J. Bremner, Bradley D. Anawalt, Alvin M. Matsumoto, John K. Amory
{"title":"Intratesticular Androgens and Spermatogenesis During Severe Gonadotropin Suppression Induced by Male Hormonal Contraceptive Treatment","authors":"Stephanie T. Page, Thomas F. Kalhorn, William J. Bremner, Bradley D. Anawalt, Alvin M. Matsumoto, John K. Amory","doi":"10.2164/jandrol.107.002790","DOIUrl":null,"url":null,"abstract":"<p><b>ABSTRACT: </b> Male hormonal contraceptive regimens function by suppressing gonadotropin secretion, resulting in a dramatic decrease in testicular androgen biosynthesis and spermatogenesis. Animal studies suggest that persistent intratesticular <i>(iT)</i>-androgen production has a stimulatory effect on spermatogenesis in the setting of gonadotropin suppression. We hypothesized that men with incompletely suppressed spermatogenesis (>1 000 000 sperm/mL) during male hormonal contraceptive treatment would have higher <i>iT</i>-androgen concentrations than men who achieved severe oligospermia (≤1 000 000 sperm/mL). Twenty healthy men ages 18–55 years enrolled in a 6-month male contraceptive study of transdermal testosterone (T) gel (100 mg/d) plus depomedroxyprogesterone acetate (300 mg intramuscularly every 12 weeks) with or without the gonadotropin releasing hormone (GnRH) antagonist acyline (300 μg/kg subcutaneously every 2 weeks for 12 weeks) were studied. During the 24th week of treatment, subjects underwent fine needle aspirations of the testes and <i>iT</i>-T and <i>iT</i>-dihydrotestosterone (<i>iT</i>-DHT) were measured in testicular fluid by liquid chromatography—tandem mass spectrometry. All men dramatically suppressed spermatogenesis; 15 of 20 men were severely oligospermic, and 5 of 20 suppressed to 1.5 million −3.2 million sperm per milliliter. In all subjects, mean <i>iT</i>-T and <i>iT</i>-DHT concentrations were 35 ± 8 and 5.1 ± 0.8 nmol/L. <i>IT</i>-androgen concentrations did not significantly differ in men who did and did not achieve severe oligospermia (<i>P</i> = .41 for <i>iT</i>-T; <i>P</i> = .18 for <i>iT</i>-DHT). Furthermore, there was no significant correlation between <i>iT</i>-T or <i>iT</i>-DHT and sperm concentration after 24 weeks of treatment. In this study of prolonged gonadotropin suppression induced by male hormonal contraceptive treatment, differences in <i>iT</i>-androgens did not explain differences in spermatogenesis. Additional studies to identify factors involved in persistent spermatogenesis despite gonadotropin suppression are warranted.</p>","PeriodicalId":15029,"journal":{"name":"Journal of andrology","volume":"28 5","pages":"734-741"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2164/jandrol.107.002790","citationCount":"40","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of andrology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.2164/jandrol.107.002790","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 40
Abstract
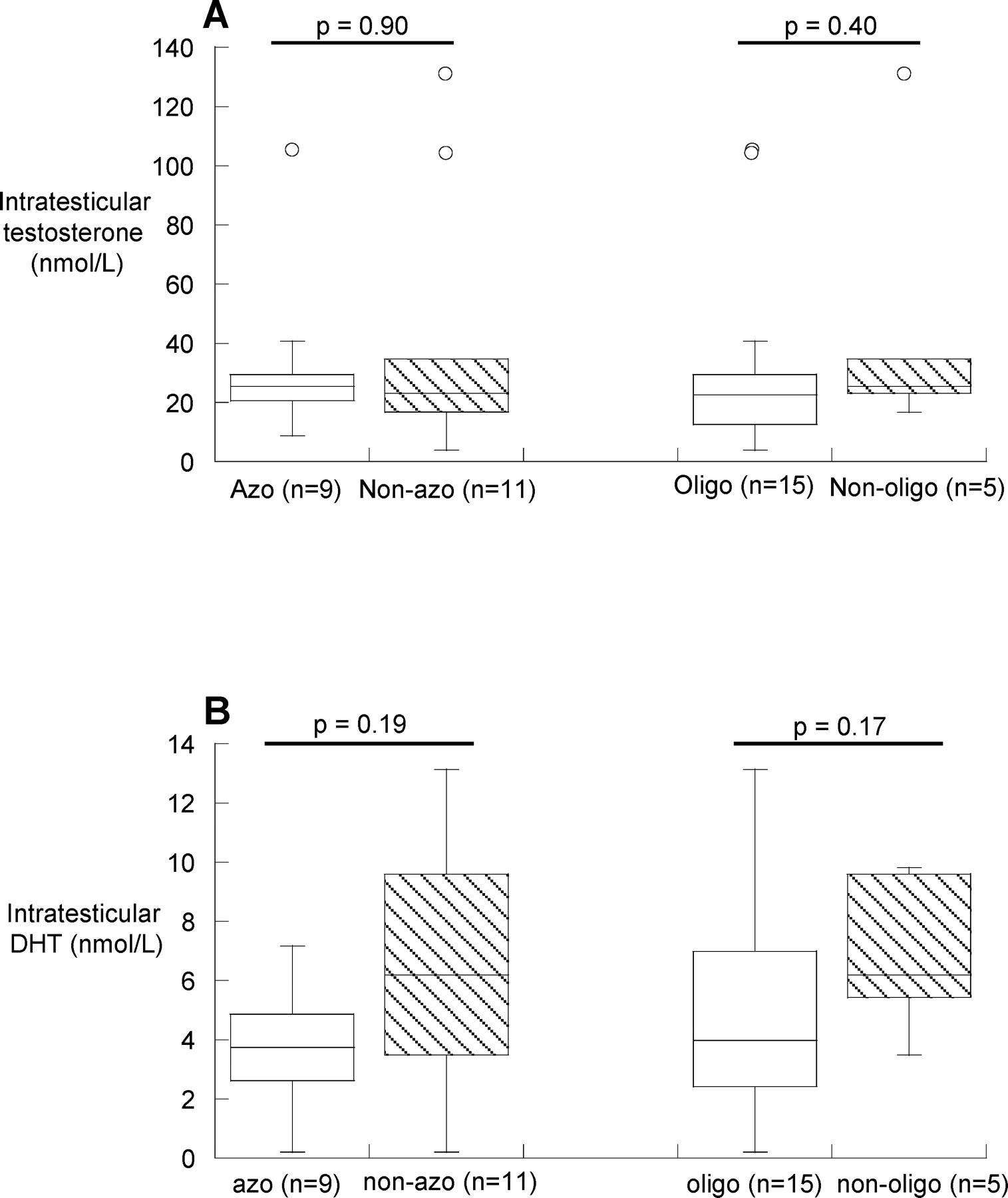
ABSTRACT: Male hormonal contraceptive regimens function by suppressing gonadotropin secretion, resulting in a dramatic decrease in testicular androgen biosynthesis and spermatogenesis. Animal studies suggest that persistent intratesticular (iT)-androgen production has a stimulatory effect on spermatogenesis in the setting of gonadotropin suppression. We hypothesized that men with incompletely suppressed spermatogenesis (>1 000 000 sperm/mL) during male hormonal contraceptive treatment would have higher iT-androgen concentrations than men who achieved severe oligospermia (≤1 000 000 sperm/mL). Twenty healthy men ages 18–55 years enrolled in a 6-month male contraceptive study of transdermal testosterone (T) gel (100 mg/d) plus depomedroxyprogesterone acetate (300 mg intramuscularly every 12 weeks) with or without the gonadotropin releasing hormone (GnRH) antagonist acyline (300 μg/kg subcutaneously every 2 weeks for 12 weeks) were studied. During the 24th week of treatment, subjects underwent fine needle aspirations of the testes and iT-T and iT-dihydrotestosterone (iT-DHT) were measured in testicular fluid by liquid chromatography—tandem mass spectrometry. All men dramatically suppressed spermatogenesis; 15 of 20 men were severely oligospermic, and 5 of 20 suppressed to 1.5 million −3.2 million sperm per milliliter. In all subjects, mean iT-T and iT-DHT concentrations were 35 ± 8 and 5.1 ± 0.8 nmol/L. IT-androgen concentrations did not significantly differ in men who did and did not achieve severe oligospermia (P = .41 for iT-T; P = .18 for iT-DHT). Furthermore, there was no significant correlation between iT-T or iT-DHT and sperm concentration after 24 weeks of treatment. In this study of prolonged gonadotropin suppression induced by male hormonal contraceptive treatment, differences in iT-androgens did not explain differences in spermatogenesis. Additional studies to identify factors involved in persistent spermatogenesis despite gonadotropin suppression are warranted.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
