{"title":"Comparison of renal effects of ibuprofen versus indomethacin during treatment of patent ductus arteriosus in contiguous historical cohorts.","authors":"Alla Kushnir, Joaquim Mb Pinheiro","doi":"10.1186/1472-6904-11-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ibuprofen treatment of patent ductus arteriosus (PDA) has been shown to be as effective as indomethacin in small randomized controlled trials, with possibly fewer adverse effects. However, adverse renal effects of ibuprofen have been noted in some trials and suspected in our practice.The purpose of this study was to examine whether ibuprofen and indomethacin treatment of PDA have comparable effects on renal function as evidenced by urine output and serum creatinine.</p><p><strong>Methods: </strong>Retrospective chart review of 350 patients. Serum creatinine and urine output were recorded prior to start of treatment, during each course and after the last course of treatment. Pre-treatment mean creatinine and urine output values were compared to treatment and post treatment means using 2-factor repeated measures ANOVA.</p><p><strong>Results: </strong>165 patients were treated with indomethacin (2005-2006) and 185 received ibuprofen (2007-2008). There was no difference between treatment groups in demographics or baseline renal function. For both groups, the number of treatment courses was inversely correlated with birth weight and gestational age. Analysis of the first course including all patients, revealed significant increase in creatinine and decrease in urine output with both drugs, with a more pronounced effect of indomethacin on creatinine. In the subgroup of 219 patients who received only one treatment course, there was a significant increase in creatinine after indomethacin, but not after ibuprofen. In the 131 who received 2 or more courses, the decrease in urine output and increase in creatinine were not different between drugs. There were significant decreases in urine output observed in the second and third courses of ibuprofen treatment (both by 0.9 mL/kg/hr).</p><p><strong>Conclusion: </strong>Both drugs have a similar short-term effect on renal function. Indomethacin had a more prominent initial effect, while ibuprofen decreased renal function during the second and third courses similarly to indomethacin. The changes in renal function seen with ibuprofen treatment should be considered in fluid and electrolyte management, especially if treatment beyond one course is required.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":"11 ","pages":"8"},"PeriodicalIF":0.0000,"publicationDate":"2011-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1472-6904-11-8","citationCount":"23","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-11-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 23
Abstract
Background: Ibuprofen treatment of patent ductus arteriosus (PDA) has been shown to be as effective as indomethacin in small randomized controlled trials, with possibly fewer adverse effects. However, adverse renal effects of ibuprofen have been noted in some trials and suspected in our practice.The purpose of this study was to examine whether ibuprofen and indomethacin treatment of PDA have comparable effects on renal function as evidenced by urine output and serum creatinine.
Methods: Retrospective chart review of 350 patients. Serum creatinine and urine output were recorded prior to start of treatment, during each course and after the last course of treatment. Pre-treatment mean creatinine and urine output values were compared to treatment and post treatment means using 2-factor repeated measures ANOVA.
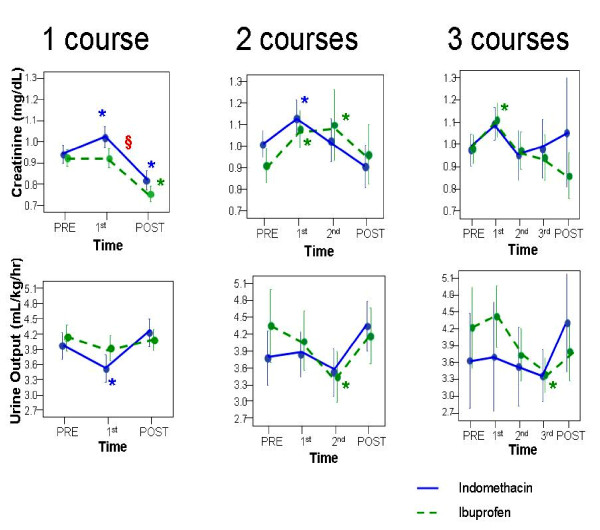
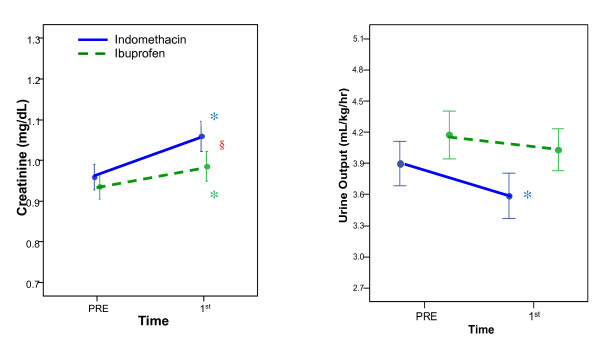
Results: 165 patients were treated with indomethacin (2005-2006) and 185 received ibuprofen (2007-2008). There was no difference between treatment groups in demographics or baseline renal function. For both groups, the number of treatment courses was inversely correlated with birth weight and gestational age. Analysis of the first course including all patients, revealed significant increase in creatinine and decrease in urine output with both drugs, with a more pronounced effect of indomethacin on creatinine. In the subgroup of 219 patients who received only one treatment course, there was a significant increase in creatinine after indomethacin, but not after ibuprofen. In the 131 who received 2 or more courses, the decrease in urine output and increase in creatinine were not different between drugs. There were significant decreases in urine output observed in the second and third courses of ibuprofen treatment (both by 0.9 mL/kg/hr).
Conclusion: Both drugs have a similar short-term effect on renal function. Indomethacin had a more prominent initial effect, while ibuprofen decreased renal function during the second and third courses similarly to indomethacin. The changes in renal function seen with ibuprofen treatment should be considered in fluid and electrolyte management, especially if treatment beyond one course is required.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
