Antoine J Cherfan, Hani M Tamim, Abdulrahman AlJumah, Asgar H Rishu, Abdulmajeed Al-Abdulkareem, Bandar A Al Knawy, Ali Hajeer, Waleed Tamimi, Riette Brits, Yaseen M Arabi
{"title":"Etomidate and mortality in cirrhotic patients with septic shock.","authors":"Antoine J Cherfan, Hani M Tamim, Abdulrahman AlJumah, Asgar H Rishu, Abdulmajeed Al-Abdulkareem, Bandar A Al Knawy, Ali Hajeer, Waleed Tamimi, Riette Brits, Yaseen M Arabi","doi":"10.1186/1472-6904-11-22","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clinical effects and outcomes of a single dose etomidate prior to intubation in the intensive care setting is controversial. The aim of this study is to evaluate the association of a single dose effect of etomidate prior to intubation on the mortality of septic cirrhotic patients and the impact of the subsequent use of low dose hydrocortisone.</p><p><strong>Methods: </strong>This is a nested-cohort study within a randomized double blind placebo controlled study evaluating the use of low dose hydrocortisone in cirrhotic septic patients. Cirrhotic septic patients ≥ 18 years were included in the study. Patients who received etomidate prior to intubation were compared to those who did not receive etomidate for all cause 28-day mortality as a primary outcome.</p><p><strong>Results: </strong>Sixty two intubated patients out of the 75 patients randomized in the initial trial were eligible for this study. Twenty three of the 62 intubated patients received etomidate dose prior to intubation. Etomidate use was not associated with all cause 28-day mortality or hospital mortality but was associated with significantly higher ICU mortality (91% vs. 64% for etomidate and controls groups, respectively; p = 0.02). Etomidate patients who received subsequent doses of hydrocortisone required lower doses of vasopressors and had more vasopressor-free days but no improvement in mortality.</p><p><strong>Conclusions: </strong>In this group of septic cirrhotic patients with very high mortality, etomidate increased ICU mortality. Subsequent use of hydrocortisone appears to have no benefit beyond decreasing vasopressor requirements. The lowest mortality was observed in patients who did not receive etomidate but received hydrocortisone.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":"11 ","pages":"22"},"PeriodicalIF":0.0000,"publicationDate":"2011-12-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1472-6904-11-22","citationCount":"19","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-11-22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 19
Abstract
Background: Clinical effects and outcomes of a single dose etomidate prior to intubation in the intensive care setting is controversial. The aim of this study is to evaluate the association of a single dose effect of etomidate prior to intubation on the mortality of septic cirrhotic patients and the impact of the subsequent use of low dose hydrocortisone.
Methods: This is a nested-cohort study within a randomized double blind placebo controlled study evaluating the use of low dose hydrocortisone in cirrhotic septic patients. Cirrhotic septic patients ≥ 18 years were included in the study. Patients who received etomidate prior to intubation were compared to those who did not receive etomidate for all cause 28-day mortality as a primary outcome.
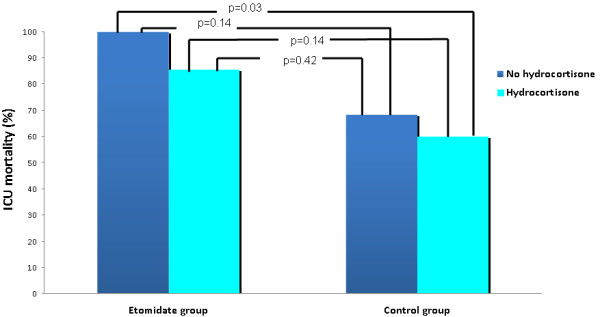
Results: Sixty two intubated patients out of the 75 patients randomized in the initial trial were eligible for this study. Twenty three of the 62 intubated patients received etomidate dose prior to intubation. Etomidate use was not associated with all cause 28-day mortality or hospital mortality but was associated with significantly higher ICU mortality (91% vs. 64% for etomidate and controls groups, respectively; p = 0.02). Etomidate patients who received subsequent doses of hydrocortisone required lower doses of vasopressors and had more vasopressor-free days but no improvement in mortality.
Conclusions: In this group of septic cirrhotic patients with very high mortality, etomidate increased ICU mortality. Subsequent use of hydrocortisone appears to have no benefit beyond decreasing vasopressor requirements. The lowest mortality was observed in patients who did not receive etomidate but received hydrocortisone.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
