Euan A Sandilands, Sharon Cameron, Frances Paterson, Sam Donaldson, Lesley Briody, Jane Crowe, Julie Donnelly, Adrian Thompson, Neil R Johnston, Ivor Mackenzie, Neal Uren, Jane Goddard, David J Webb, Ian L Megson, Nicholas Bateman, Michael Eddleston
{"title":"Mechanisms for an effect of acetylcysteine on renal function after exposure to radio-graphic contrast material: study protocol.","authors":"Euan A Sandilands, Sharon Cameron, Frances Paterson, Sam Donaldson, Lesley Briody, Jane Crowe, Julie Donnelly, Adrian Thompson, Neil R Johnston, Ivor Mackenzie, Neal Uren, Jane Goddard, David J Webb, Ian L Megson, Nicholas Bateman, Michael Eddleston","doi":"10.1186/1472-6904-12-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contrast-induced nephropathy is a common complication of contrast administration in patients with chronic kidney disease and diabetes. Its pathophysiology is not well understood; similarly the role of intravenous or oral acetylcysteine is unclear. Randomized controlled trials to date have been conducted without detailed knowledge of the effect of acetylcysteine on renal function. We are conducting a detailed mechanistic study of acetylcysteine on normal and impaired kidneys, both with and without contrast. This information would guide the choice of dose, route, and appropriate outcome measure for future clinical trials in patients with chronic kidney disease.</p><p><strong>Methods/design: </strong>We designed a 4-part study. We have set up randomised controlled cross-over studies to assess the effect of intravenous (50 mg/kg/hr for 2 hrs before contrast exposure, then 20 mg/kg/hr for 5 hrs) or oral acetylcysteine (1200 mg twice daily for 2 days, starting the day before contrast exposure) on renal function in normal and diseased kidneys, and normal kidneys exposed to contrast. We have also set up a parallel-group randomized controlled trial to assess the effect of intravenous or oral acetylcysteine on patients with chronic kidney disease stage III undergoing elective coronary angiography. The primary outcome is change in renal blood flow; secondary outcomes include change in glomerular filtration rate, tubular function, urinary proteins, and oxidative balance.</p><p><strong>Discussion: </strong>Contrast-induced nephropathy represents a significant source of hospital morbidity and mortality. Over the last ten years, acetylcysteine has been administered prior to contrast to reduce the risk of contrast-induced nephropathy. Randomized controlled trials, however, have not reliably demonstrated renoprotection; a recent large randomized controlled trial assessing a dose of oral acetylcysteine selected without mechanistic insight did not reduce the incidence of contrast-induced nephropathy. Our study should reveal the mechanism of effect of acetylcysteine on renal function and identify an appropriate route for future dose response studies and in time randomized controlled trials.</p><p><strong>Trial registration: </strong>Clinical Trials.gov: NCT00558142; EudraCT: 2006-003509-18.</p>","PeriodicalId":9196,"journal":{"name":"BMC Clinical Pharmacology","volume":"12 ","pages":"3"},"PeriodicalIF":0.0000,"publicationDate":"2012-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3293780/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1472-6904-12-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Contrast-induced nephropathy is a common complication of contrast administration in patients with chronic kidney disease and diabetes. Its pathophysiology is not well understood; similarly the role of intravenous or oral acetylcysteine is unclear. Randomized controlled trials to date have been conducted without detailed knowledge of the effect of acetylcysteine on renal function. We are conducting a detailed mechanistic study of acetylcysteine on normal and impaired kidneys, both with and without contrast. This information would guide the choice of dose, route, and appropriate outcome measure for future clinical trials in patients with chronic kidney disease.
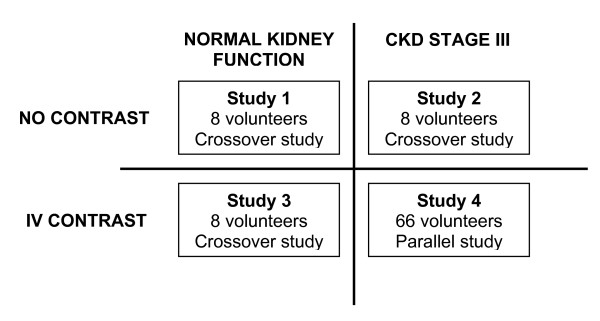
Methods/design: We designed a 4-part study. We have set up randomised controlled cross-over studies to assess the effect of intravenous (50 mg/kg/hr for 2 hrs before contrast exposure, then 20 mg/kg/hr for 5 hrs) or oral acetylcysteine (1200 mg twice daily for 2 days, starting the day before contrast exposure) on renal function in normal and diseased kidneys, and normal kidneys exposed to contrast. We have also set up a parallel-group randomized controlled trial to assess the effect of intravenous or oral acetylcysteine on patients with chronic kidney disease stage III undergoing elective coronary angiography. The primary outcome is change in renal blood flow; secondary outcomes include change in glomerular filtration rate, tubular function, urinary proteins, and oxidative balance.
Discussion: Contrast-induced nephropathy represents a significant source of hospital morbidity and mortality. Over the last ten years, acetylcysteine has been administered prior to contrast to reduce the risk of contrast-induced nephropathy. Randomized controlled trials, however, have not reliably demonstrated renoprotection; a recent large randomized controlled trial assessing a dose of oral acetylcysteine selected without mechanistic insight did not reduce the incidence of contrast-induced nephropathy. Our study should reveal the mechanism of effect of acetylcysteine on renal function and identify an appropriate route for future dose response studies and in time randomized controlled trials.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
