Pasquale Niscola, Massimiliano Palombi, Stefano Fratoni, Malgorzata Monika Trawinska, Laura Scaramucci, Andrea Tendas, Marco Giovannini, Alessio Perrotti, Paolo de Fabritiis
{"title":"Long-term survival of a patient with bone marrow gelatinous degeneration of idiopathic origin.","authors":"Pasquale Niscola, Massimiliano Palombi, Stefano Fratoni, Malgorzata Monika Trawinska, Laura Scaramucci, Andrea Tendas, Marco Giovannini, Alessio Perrotti, Paolo de Fabritiis","doi":"10.5045/kjh.2012.47.4.309","DOIUrl":null,"url":null,"abstract":"TO THE EDITOR: Gelatinous bone marrow transformation (GMT) is a rare bone marrow (BM) disorder of unknown pathogenesis. It is characterized by fat cell atrophy, focal loss of hematopoietic cells, and deposition of extracellular gelatinous substances (mucopolysaccharides rich in hyaluronic acid) [1]. The pathogenesis of GMT involves the deposition of hyaluronic acid, which hampers hematopoiesis by altering the BM microenvironment and stroma and disruption of the interactions between BM cells and cell signaling molecules [1]. GMT has been reported in association with chronic debilitating diseases, such as anorexia nervosa, malnutrition, and human immunodeficiency virus (HIV) infection, and after cytotoxic treatments [2]; in addition, GMT has been described in patients with myelodysplastic syndrome [3], acute myeloblastic leukemia [3], and idiopathic myelofibrosis [4]. However, idiopathic GMT has also been reported [5]. Herein, we report a case of idiopathic GMT in a patient who had an unusual clinical course and long-term survival. The patient was a 64-year-old Caribbean woman who had been living in Rome for more than 30 years. She was referred to our clinic in December 2005 because of anemia. Her past medical history was unremarkable. She did not use alcohol, drugs, or tobacco, and her nutritional status was excellent. Physical examination was unremarkable with the exception of pallor; the patient did not have either spleen or liver enlargement. A complete blood count at admission showed normochromic-normocytic anemia with reticulocytopenia and normal white blood cell and platelet counts. Total and unconjugated bilirubin and serum haptoglobin levels were normal. Direct and indirect indirect Coombs tests were negative. Serological tests for HIV, cytomegalovirus, Epstein-Barr virus, parvovirus B19, and hepatitis B and C viruses were negative. In addition, serum levels of tri-iodothyronine were normal. Moreover, no clinical or laboratory features of autoimmune disease were detected. Examination of peripheral blood smears revealed normal RBC; erythrocyte fragments were not detectable. Radiological examinations, which included a whole-body computed tomography scan, revealed no abnormalities. Occult blood loss was ruled out by fecal and urine analyses. A BM aspirate performed at admission resulted in a dry tap. Therefore, a BM trephine biopsy was taken. Histological examination of the BM sample revealed GMT (Fig. 1). The patient did not respond to any potentially disease-modifying treatment, including erythropoietin, prednisone, and cyclosporine. Therefore, she was managed with supportive measures, primarily transfusions. The clinical course was uncomplicated and her hematological status has remained stable. To date, 80 months after the diagnosis, she is managed only with supportive measures, consisting of 2 units of packed RBC every 3 weeks, along with iron chelation therapy. In addition, her BM features, which have been evaluated annually by BM trephine biopsies, have remained stable. In conclusion, we have described a case of an apparently healthy woman who presented with GMT approximately 7 years ago, in whom anemia was the only clinical manifestation of hematopoietic impairment. To the best of our knowledge, no such case of GMT has been reported previously as an idiopathic primary condition. \n \n \n \nFig. 1 \n \nSerous atrophy in a diffuse and severe hypocellular background (A). Reduced fat cells, a diffuse extracellular gelatinous amorphous material, small typical lymphocytes, and mature plasma cells were also observed (B). Small islets of hematopoietic cells ...","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"47 4","pages":"309-10"},"PeriodicalIF":0.0000,"publicationDate":"2012-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2012.47.4.309","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2012.47.4.309","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/12/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
TO THE EDITOR: Gelatinous bone marrow transformation (GMT) is a rare bone marrow (BM) disorder of unknown pathogenesis. It is characterized by fat cell atrophy, focal loss of hematopoietic cells, and deposition of extracellular gelatinous substances (mucopolysaccharides rich in hyaluronic acid) [1]. The pathogenesis of GMT involves the deposition of hyaluronic acid, which hampers hematopoiesis by altering the BM microenvironment and stroma and disruption of the interactions between BM cells and cell signaling molecules [1]. GMT has been reported in association with chronic debilitating diseases, such as anorexia nervosa, malnutrition, and human immunodeficiency virus (HIV) infection, and after cytotoxic treatments [2]; in addition, GMT has been described in patients with myelodysplastic syndrome [3], acute myeloblastic leukemia [3], and idiopathic myelofibrosis [4]. However, idiopathic GMT has also been reported [5]. Herein, we report a case of idiopathic GMT in a patient who had an unusual clinical course and long-term survival. The patient was a 64-year-old Caribbean woman who had been living in Rome for more than 30 years. She was referred to our clinic in December 2005 because of anemia. Her past medical history was unremarkable. She did not use alcohol, drugs, or tobacco, and her nutritional status was excellent. Physical examination was unremarkable with the exception of pallor; the patient did not have either spleen or liver enlargement. A complete blood count at admission showed normochromic-normocytic anemia with reticulocytopenia and normal white blood cell and platelet counts. Total and unconjugated bilirubin and serum haptoglobin levels were normal. Direct and indirect indirect Coombs tests were negative. Serological tests for HIV, cytomegalovirus, Epstein-Barr virus, parvovirus B19, and hepatitis B and C viruses were negative. In addition, serum levels of tri-iodothyronine were normal. Moreover, no clinical or laboratory features of autoimmune disease were detected. Examination of peripheral blood smears revealed normal RBC; erythrocyte fragments were not detectable. Radiological examinations, which included a whole-body computed tomography scan, revealed no abnormalities. Occult blood loss was ruled out by fecal and urine analyses. A BM aspirate performed at admission resulted in a dry tap. Therefore, a BM trephine biopsy was taken. Histological examination of the BM sample revealed GMT (Fig. 1). The patient did not respond to any potentially disease-modifying treatment, including erythropoietin, prednisone, and cyclosporine. Therefore, she was managed with supportive measures, primarily transfusions. The clinical course was uncomplicated and her hematological status has remained stable. To date, 80 months after the diagnosis, she is managed only with supportive measures, consisting of 2 units of packed RBC every 3 weeks, along with iron chelation therapy. In addition, her BM features, which have been evaluated annually by BM trephine biopsies, have remained stable. In conclusion, we have described a case of an apparently healthy woman who presented with GMT approximately 7 years ago, in whom anemia was the only clinical manifestation of hematopoietic impairment. To the best of our knowledge, no such case of GMT has been reported previously as an idiopathic primary condition.
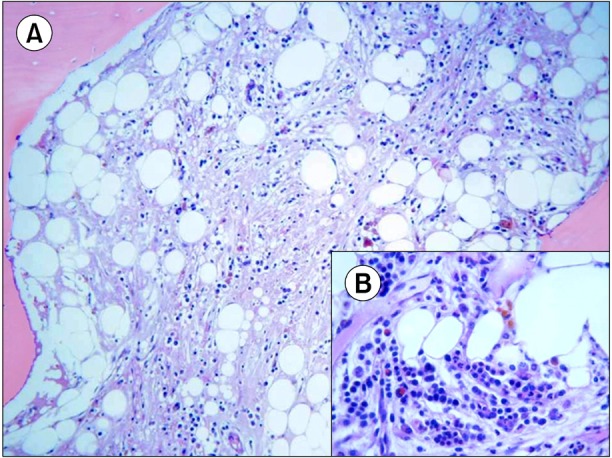
Fig. 1
Serous atrophy in a diffuse and severe hypocellular background (A). Reduced fat cells, a diffuse extracellular gelatinous amorphous material, small typical lymphocytes, and mature plasma cells were also observed (B). Small islets of hematopoietic cells ...


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
