Min Jin Kim, John Jeongseok Yang, Claus Meyer, Rolf Marschalek, Tae Sung Park
{"title":"Molecular methods for genomic analyses of variant PML-RARA or other RARA-related chromosomal translocations in acute promyelocytic leukemia.","authors":"Min Jin Kim, John Jeongseok Yang, Claus Meyer, Rolf Marschalek, Tae Sung Park","doi":"10.5045/kjh.2012.47.4.307","DOIUrl":null,"url":null,"abstract":"TO THE EDITOR: We read an interesting paper by Palta et al. in a recent issue of the Korean Journal of Hematology titled, \"ZBTB16-RARA variant of acute promyelocytic leukemia with tuberculosis: a case report and review of literature\" [1]. We would like to add some comments to their article and suggest additional molecular methods to confirm variant translocations in acute promyelocytic leukemia (APL). \n \nApart from its characteristic morphology, APL is strongly correlated with presence of the PML-RARA fusion gene due to a t(15;17) translocation. Patients displaying cryptic PML-RARA gene rearrangements or other translocations involving RARA are very rare. Since RARA generates chimeric fusion genes with various partners such as ZBTB16 at 11q23, NUMA1 at 11q13, NPM1 at 5q35, FIP1L1 at 4q12, and STAT5b at 17q11.2 (Fig. 1), confirmatory molecular methods to detect gene rearrangements are necessary when unique or unusual chromosomal translocations are found in APL cases. Palta et al. reported a case of APL accompanied by tuberculosis where cytogenetic study showed a variant chromosomal translocation, t(11;17)(q23;q21). First, although they describe this case as APL with t(11;17)(q23;q21) through bone marrow (BM), immunophenotyping, and cytogenetic studies, we noted an absence of results based on molecular methods. To demonstrate the existence of the ZBTB16-RARA fusion gene, a single specific reverse transcriptase-polymerase chain reaction (RT-PCR) with a specific primer to detect the gene rearrangement or multiplex RT-PCR (e.g. HemaVision) to detect ZBTB16-RARA could have provided an accurate molecular diagnostic result. Second, the authors' reference to a paper by Kang et al. was puzzling despite the fact that it was cited as a similar case with chromosomal translocations at a similar location, in cases of AML with chromosomal translocation t(11;17) [2]. In the first case, cytogenetic analysis from BM aspirate showed t(11;17)(q23;q21) in 18 out of 20 cells while the MLL probe in fluorescence in situ hybridization (FISH) showed split-out signals in 98.5% of interphase cells. The second case also showed t(11;17)(q23;q25) in the chromosome study while the FISH assay showed split-out signals in 79% of interphase cells. However, normal fluorescence patterns were found in 200 cells in additional FISH assays when a dual-color single-fusion PML-RARA probe was used for both cases, which led to the conclusion that the MLL gene was involved in the 11q23 breakpoint and RARA was not involved in the 17q breakpoint. Hence, the authors' citation of this study to explain the ZBTB16-RARA fusion gene appears inadequate, and a molecular study could unambiguously identify the involvement of ZBTB16 at 11q23 in their case. \n \n \n \nFig. 1 \n \nVarious RARA partner genes in acute promyelocytic leukemias. \n \n \n \nWe suggest the authors conduct RT-PCR analysis of the ZBTB16-RARA fusion gene if any remnant RNA or cDNA samples from their APL patient are available. However, if only genomic DNA is available, analyzing the genomic breakpoints by multiplex long distance-polymerase chain reaction (LD-PCR) would be helpful. LD-PCR or long distance inverse (LDI)-PCR can identify known or unknown partner genes, monitor minimal residual disease (MRD), and identify multi-way chromosomal translocations such as three-way or four-way translocations [3]. We have recently used LD-PCR to confirm APL cases showing unusual karyotypes or discrepant results between conventional cytogenetics and molecular studies. More precisely, we identified a novel PML-ADAMTS17-RARA rearrangement and confirmed the genomic fusion breakpoints of cryptic PML-RARA rearrangement in 2 APL patients [3-5]. \n \nIn conclusion, detection of leukemia-associated fusion genes is important due to their direct relevance to diagnosis, MRD assessment, and treatment response. Since APL patients with ZBTB16-RARA are resistant to all-trans-retinoic acid (ATRA), molecular methods with higher resolution than chromosome studies must be conducted to detect fusion genes and facilitate selection of the most appropriate treatment. We believe that molecular techniques such as FISH, RT-PCR, and LD-PCR should be used in addition to morphology and cytogenetic studies in APL diagnosis and evaluation so that atypical PML-RARA or RARA variant gene rearrangements are not missed.","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"47 4","pages":"307-8"},"PeriodicalIF":0.0000,"publicationDate":"2012-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2012.47.4.307","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2012.47.4.307","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/12/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
TO THE EDITOR: We read an interesting paper by Palta et al. in a recent issue of the Korean Journal of Hematology titled, "ZBTB16-RARA variant of acute promyelocytic leukemia with tuberculosis: a case report and review of literature" [1]. We would like to add some comments to their article and suggest additional molecular methods to confirm variant translocations in acute promyelocytic leukemia (APL).
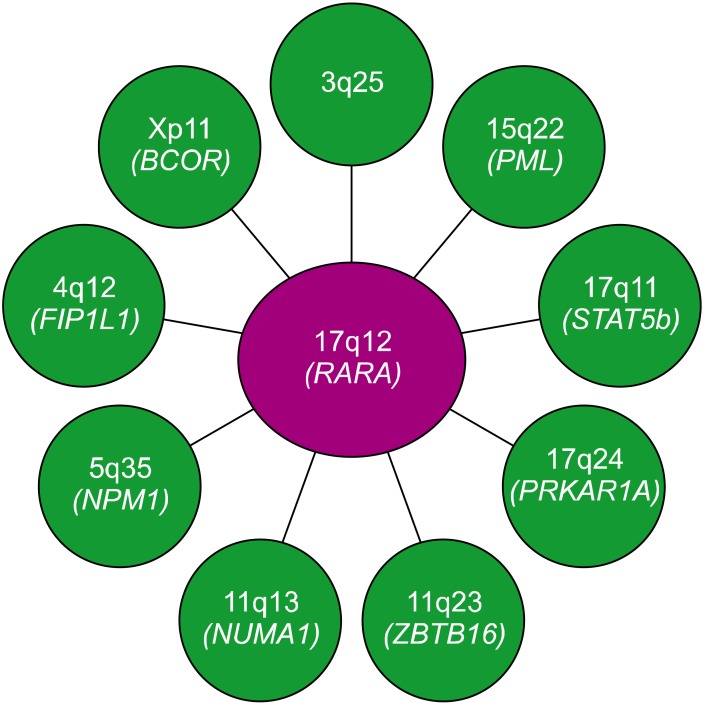
Apart from its characteristic morphology, APL is strongly correlated with presence of the PML-RARA fusion gene due to a t(15;17) translocation. Patients displaying cryptic PML-RARA gene rearrangements or other translocations involving RARA are very rare. Since RARA generates chimeric fusion genes with various partners such as ZBTB16 at 11q23, NUMA1 at 11q13, NPM1 at 5q35, FIP1L1 at 4q12, and STAT5b at 17q11.2 (Fig. 1), confirmatory molecular methods to detect gene rearrangements are necessary when unique or unusual chromosomal translocations are found in APL cases. Palta et al. reported a case of APL accompanied by tuberculosis where cytogenetic study showed a variant chromosomal translocation, t(11;17)(q23;q21). First, although they describe this case as APL with t(11;17)(q23;q21) through bone marrow (BM), immunophenotyping, and cytogenetic studies, we noted an absence of results based on molecular methods. To demonstrate the existence of the ZBTB16-RARA fusion gene, a single specific reverse transcriptase-polymerase chain reaction (RT-PCR) with a specific primer to detect the gene rearrangement or multiplex RT-PCR (e.g. HemaVision) to detect ZBTB16-RARA could have provided an accurate molecular diagnostic result. Second, the authors' reference to a paper by Kang et al. was puzzling despite the fact that it was cited as a similar case with chromosomal translocations at a similar location, in cases of AML with chromosomal translocation t(11;17) [2]. In the first case, cytogenetic analysis from BM aspirate showed t(11;17)(q23;q21) in 18 out of 20 cells while the MLL probe in fluorescence in situ hybridization (FISH) showed split-out signals in 98.5% of interphase cells. The second case also showed t(11;17)(q23;q25) in the chromosome study while the FISH assay showed split-out signals in 79% of interphase cells. However, normal fluorescence patterns were found in 200 cells in additional FISH assays when a dual-color single-fusion PML-RARA probe was used for both cases, which led to the conclusion that the MLL gene was involved in the 11q23 breakpoint and RARA was not involved in the 17q breakpoint. Hence, the authors' citation of this study to explain the ZBTB16-RARA fusion gene appears inadequate, and a molecular study could unambiguously identify the involvement of ZBTB16 at 11q23 in their case.
Fig. 1
Various RARA partner genes in acute promyelocytic leukemias.
We suggest the authors conduct RT-PCR analysis of the ZBTB16-RARA fusion gene if any remnant RNA or cDNA samples from their APL patient are available. However, if only genomic DNA is available, analyzing the genomic breakpoints by multiplex long distance-polymerase chain reaction (LD-PCR) would be helpful. LD-PCR or long distance inverse (LDI)-PCR can identify known or unknown partner genes, monitor minimal residual disease (MRD), and identify multi-way chromosomal translocations such as three-way or four-way translocations [3]. We have recently used LD-PCR to confirm APL cases showing unusual karyotypes or discrepant results between conventional cytogenetics and molecular studies. More precisely, we identified a novel PML-ADAMTS17-RARA rearrangement and confirmed the genomic fusion breakpoints of cryptic PML-RARA rearrangement in 2 APL patients [3-5].
In conclusion, detection of leukemia-associated fusion genes is important due to their direct relevance to diagnosis, MRD assessment, and treatment response. Since APL patients with ZBTB16-RARA are resistant to all-trans-retinoic acid (ATRA), molecular methods with higher resolution than chromosome studies must be conducted to detect fusion genes and facilitate selection of the most appropriate treatment. We believe that molecular techniques such as FISH, RT-PCR, and LD-PCR should be used in addition to morphology and cytogenetic studies in APL diagnosis and evaluation so that atypical PML-RARA or RARA variant gene rearrangements are not missed.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
