{"title":"Hydronephrosis in infants and children: natural history and risk factors for persistence in children followed by a medical service.","authors":"Kristy Vandervoort, Stephanie Lasky, Christine Sethna, Rachel Frank, Suzanne Vento, Jeanne Choi-Rosen, Beatrice Goilav, Howard Trachtman","doi":"10.4137/cmped.s3584","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Infants with neonatal hydronephrosis and a normal voiding cystourethrogram (VCUG) are presumed to have ureteropelvic junction obstruction (UPJO). There is little current information about the natural history of children with hydronephrosis or clinical factors that predict resolution of the radiological abnormality.</p><p><strong>Objective: </strong>To determine the time course until spontaneous resolution of neonatal hydronephrosis and define risk factors for persistence of the abnormality.</p><p><strong>Methods: </strong>This retrospective single center review examined infants and children <5 years of age with hydronephrosis who were followed for at least 12 months.</p><p><strong>Results: </strong>136 children were identified (96 male:40 female). The mean age at diagnosis of hydronephrosis was 3.3 ± 9.7 months and 76% of the patients were diagnosed at birth. The hydronephrosis was unilateral in 98 (72%) of cases, and hydronephrosis was at least moderate in severity in 22% of affected kidneys. At last follow-up at 30 ± 10 months, the abnormality had resolved in 77 out of 115 (67%) available patients, 30 (26%) had been referred to urology, and 12 (10%) had persistent hydronephrosis. Severity of hydronephrosis was the only clinical feature that predicted persistence of the abnormality (P < 0.001). There was an association between detection at birth and lack of resolution of hydronephrosis.</p><p><strong>Conclusions: </strong>Children with hydronephrosis and presumed UPJO and normal kidney parenchyma can be followed for at least 2 years to allow for spontaneous resolution before referral to urology. Serial sonography can be performed at 6 month intervals in uncomplicated cases. More severe hydronephrosis and presence of the lesion at birth may predict infants and children requiring closer observation and referral for possible surgical correction of the hydronephrosis.</p>","PeriodicalId":88452,"journal":{"name":"Clinical medicine. Pediatrics","volume":"3 ","pages":"63-70"},"PeriodicalIF":0.0000,"publicationDate":"2009-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4137/cmped.s3584","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical medicine. Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4137/cmped.s3584","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2009/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 9
Abstract
Background: Infants with neonatal hydronephrosis and a normal voiding cystourethrogram (VCUG) are presumed to have ureteropelvic junction obstruction (UPJO). There is little current information about the natural history of children with hydronephrosis or clinical factors that predict resolution of the radiological abnormality.
Objective: To determine the time course until spontaneous resolution of neonatal hydronephrosis and define risk factors for persistence of the abnormality.
Methods: This retrospective single center review examined infants and children <5 years of age with hydronephrosis who were followed for at least 12 months.
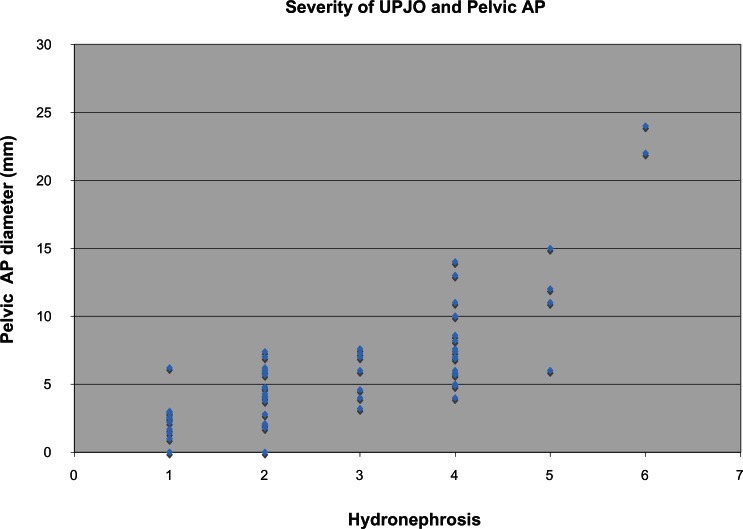
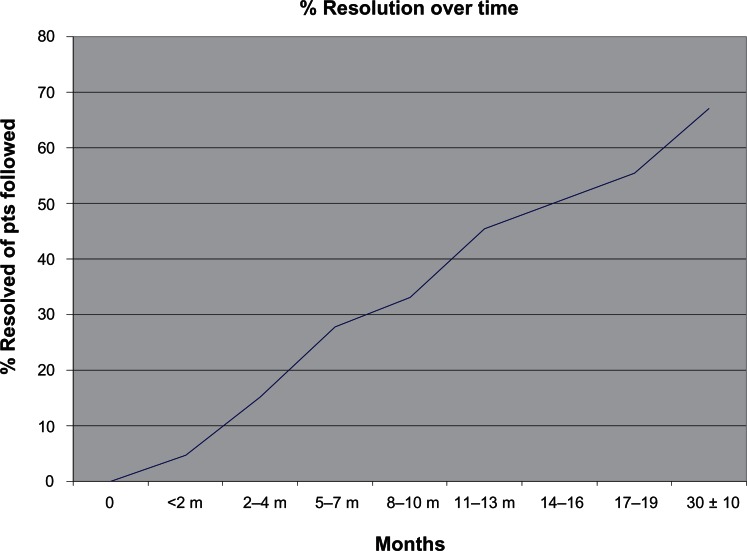
Results: 136 children were identified (96 male:40 female). The mean age at diagnosis of hydronephrosis was 3.3 ± 9.7 months and 76% of the patients were diagnosed at birth. The hydronephrosis was unilateral in 98 (72%) of cases, and hydronephrosis was at least moderate in severity in 22% of affected kidneys. At last follow-up at 30 ± 10 months, the abnormality had resolved in 77 out of 115 (67%) available patients, 30 (26%) had been referred to urology, and 12 (10%) had persistent hydronephrosis. Severity of hydronephrosis was the only clinical feature that predicted persistence of the abnormality (P < 0.001). There was an association between detection at birth and lack of resolution of hydronephrosis.
Conclusions: Children with hydronephrosis and presumed UPJO and normal kidney parenchyma can be followed for at least 2 years to allow for spontaneous resolution before referral to urology. Serial sonography can be performed at 6 month intervals in uncomplicated cases. More severe hydronephrosis and presence of the lesion at birth may predict infants and children requiring closer observation and referral for possible surgical correction of the hydronephrosis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
