{"title":"Novel strategies in glioblastoma surgery aim at safe, supra-maximum resection in conjunction with local therapies.","authors":"John G Wolbers","doi":"10.5732/cjc.013.10219","DOIUrl":null,"url":null,"abstract":"<p><p>The biggest challenge in neuro-oncology is the treatment of glioblastoma, which exhibits poor prognosis and is increasing in incidence in an increasing aging population. Diverse treatment strategies aim at maximum cytoreduction and ensuring good quality of life. We discuss multimodal neuronavigation, supra-maximum tumor resection, and the postoperative treatment gap. Multimodal neuronavigation allows the integration of preoperative anatomic and functional data with intraoperative information. This approach includes functional magnetic resonance imaging (MRI) and diffusion tensor imaging in preplanning and ultrasound, computed tomography (CT), MRI and direct (sub)cortical stimulation during surgery. The practice of awake craniotomy decreases postoperative neurologic deficits, and an extensive supra-maximum resection appears to be feasible, even in eloquent areas of the brain. Intraoperative MRI- and fluorescence-guided surgery assist in achieving this goal of supra-maximum resection and have been the subject of an increasing number of reports. Photodynamic therapy and local chemotherapy are properly positioned to bridge the gap between surgery and chemoradiotherapy. The photosensitizer used in fluorescence-guided surgery persists in the remaining peripheral tumor extensions. Additionally, blinded randomized clinical trials showed firm evidence of extra cytoreduction by local chemotherapy in the tumor cavity. The cutting-edge promise is gene therapy although both the delivery and efficacy of the numerous transgenes remain under investigation. Issues such as the choice of (cell) vector, the choice of therapeutic transgene, the optimal route of administration, and biosafety need to be addressed in a systematic way. In this selective review, we present various evidence and promises to improve survival of glioblastoma patients by supra-maximum cytoreduction via local procedures while minimizing the risk of new neurologic deficit. </p>","PeriodicalId":10034,"journal":{"name":"癌症","volume":"33 1","pages":"8-15"},"PeriodicalIF":0.0000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5732/cjc.013.10219","citationCount":"29","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"癌症","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5732/cjc.013.10219","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 29
Abstract
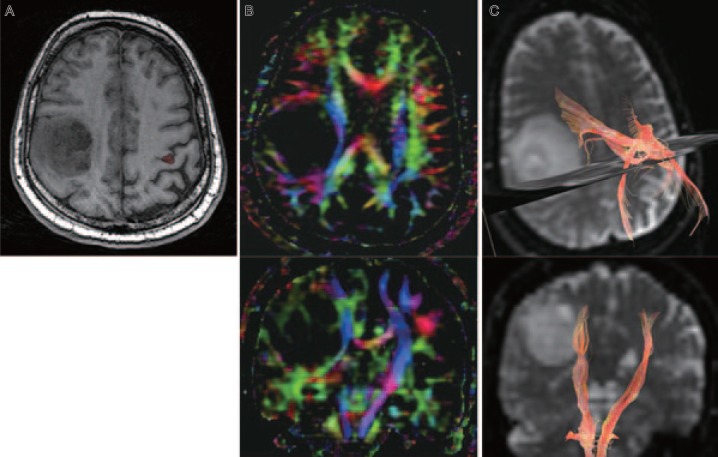
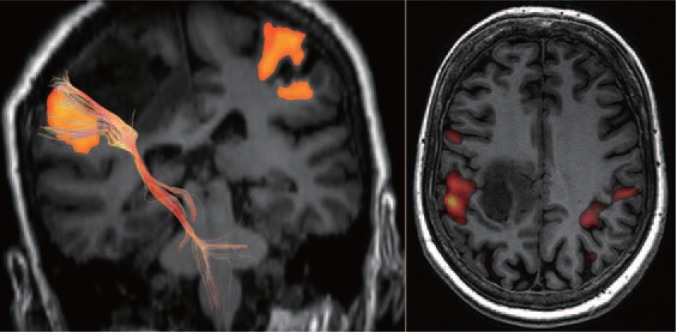
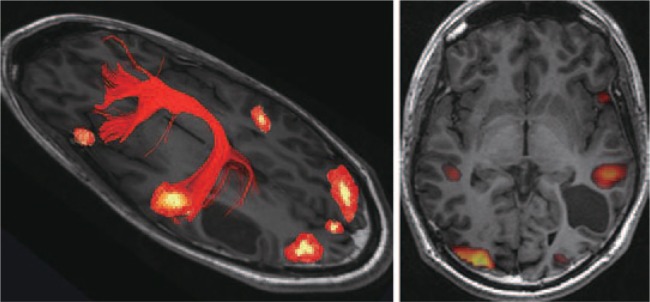
The biggest challenge in neuro-oncology is the treatment of glioblastoma, which exhibits poor prognosis and is increasing in incidence in an increasing aging population. Diverse treatment strategies aim at maximum cytoreduction and ensuring good quality of life. We discuss multimodal neuronavigation, supra-maximum tumor resection, and the postoperative treatment gap. Multimodal neuronavigation allows the integration of preoperative anatomic and functional data with intraoperative information. This approach includes functional magnetic resonance imaging (MRI) and diffusion tensor imaging in preplanning and ultrasound, computed tomography (CT), MRI and direct (sub)cortical stimulation during surgery. The practice of awake craniotomy decreases postoperative neurologic deficits, and an extensive supra-maximum resection appears to be feasible, even in eloquent areas of the brain. Intraoperative MRI- and fluorescence-guided surgery assist in achieving this goal of supra-maximum resection and have been the subject of an increasing number of reports. Photodynamic therapy and local chemotherapy are properly positioned to bridge the gap between surgery and chemoradiotherapy. The photosensitizer used in fluorescence-guided surgery persists in the remaining peripheral tumor extensions. Additionally, blinded randomized clinical trials showed firm evidence of extra cytoreduction by local chemotherapy in the tumor cavity. The cutting-edge promise is gene therapy although both the delivery and efficacy of the numerous transgenes remain under investigation. Issues such as the choice of (cell) vector, the choice of therapeutic transgene, the optimal route of administration, and biosafety need to be addressed in a systematic way. In this selective review, we present various evidence and promises to improve survival of glioblastoma patients by supra-maximum cytoreduction via local procedures while minimizing the risk of new neurologic deficit.
期刊介绍:
In July 2008, Landes Bioscience and Sun Yat-sen University Cancer Center began co-publishing the international, English-language version of AI ZHENG or the Chinese Journal of Cancer (CJC). CJC publishes original research, reviews, extra views, perspectives, supplements, and spotlights in all areas of cancer research. The primary criteria for publication in CJC are originality, outstanding scientific merit, and general interest. The Editorial Board is composed of members from around the world, who will strive to maintain the highest standards for excellence in order to generate a valuable resource for an international readership.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
