Olufoladare G Olorunsola, Steven H Kim, Ryan Chang, Yuo-Chen Kuo, Steven W Hetts, Alex Heller, Rishi Kant, Maythem Saeed, William H Fissell, Shuvo Roy, Mark W Wilson
{"title":"Imaging assessment of a portable hemodialysis device: detection of possible failure modes and monitoring of functional performance.","authors":"Olufoladare G Olorunsola, Steven H Kim, Ryan Chang, Yuo-Chen Kuo, Steven W Hetts, Alex Heller, Rishi Kant, Maythem Saeed, William H Fissell, Shuvo Roy, Mark W Wilson","doi":"10.7243/2052-6962-2-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of this study was to investigate the utility and limitations of various imaging modalities in the noninvasive assessment of a novel compact hemodialyzer under development for renal replacement therapy, with specific aim towards monitoring its functional performance.</p><p><strong>Methods: </strong>The prototype is a 4×3×6 cm aluminum cartridge housing \"blood\" and \"dialysate\" flow paths arranged in parallel. A sheet of semipermeable silicon nanopore membranes forms the blood-dialysate interface, allowing passage of small molecules. Blood flow was simulated using a peristaltic pump to instill iodinated contrast through the blood compartment, while de-ionized water was instilled through the dialysate compartment at a matched rate in the countercurrent direction. Images were acquired under these flow conditions using multi-detector computed tomography (MDCT), fluoroscopy, high-resolution quantitative computed tomography (HR-QCT), and magnetic resonance imaging (MRI). MDCT was used to monitor contrast diffusion efficiency by plotting contrast density as a function of position along the path of flow through the cartridge during steady state infusion at 1 and 20 mL/min. Both linear and exponential regressions were used to model contrast decay along the flow path.</p><p><strong>Results: </strong>Both linear and exponential models of contrast decay appeared to be reasonable approximations, yielding similar results for contrast diffusion during a single pass through the cartridge. There was no measurable difference in contrast diffusion when comparing 1 mL/min and 20 mL/min flow rates. Fluoroscopy allowed a gross qualitative assessment of flow within the device, and revealed flow inhomogeneity within the corner of the cartridge opposite the blood inlet port. MRI and HR-QCT were both severely limited due to the paramagnetic properties and high atomic number of the target material, respectively. During testing, we encountered several causes of device malfunction, including leak formation, trapped gas, and contrast-mediated nanopore clogging. We illustrate the imaging manifestations of each.</p><p><strong>Conclusions: </strong>Despite the inherent challenges in imaging a predominantly metallic device, some modalities show potential in the non-invasive assessment of a novel compact hemodialyzer. The approaches described here could potentially be translated to device evaluation in the implanted setting.</p>","PeriodicalId":90261,"journal":{"name":"Medical instrumentation (Luton, England)","volume":"2 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2014-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.7243/2052-6962-2-2","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical instrumentation (Luton, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7243/2052-6962-2-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The purpose of this study was to investigate the utility and limitations of various imaging modalities in the noninvasive assessment of a novel compact hemodialyzer under development for renal replacement therapy, with specific aim towards monitoring its functional performance.
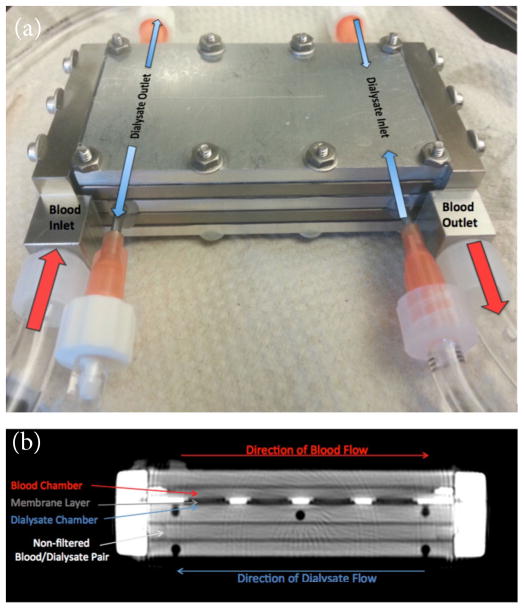
Methods: The prototype is a 4×3×6 cm aluminum cartridge housing "blood" and "dialysate" flow paths arranged in parallel. A sheet of semipermeable silicon nanopore membranes forms the blood-dialysate interface, allowing passage of small molecules. Blood flow was simulated using a peristaltic pump to instill iodinated contrast through the blood compartment, while de-ionized water was instilled through the dialysate compartment at a matched rate in the countercurrent direction. Images were acquired under these flow conditions using multi-detector computed tomography (MDCT), fluoroscopy, high-resolution quantitative computed tomography (HR-QCT), and magnetic resonance imaging (MRI). MDCT was used to monitor contrast diffusion efficiency by plotting contrast density as a function of position along the path of flow through the cartridge during steady state infusion at 1 and 20 mL/min. Both linear and exponential regressions were used to model contrast decay along the flow path.
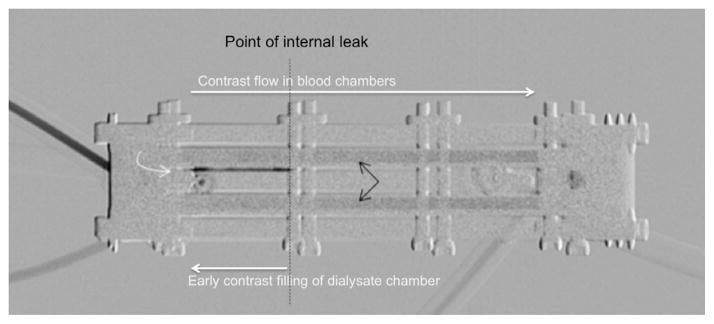
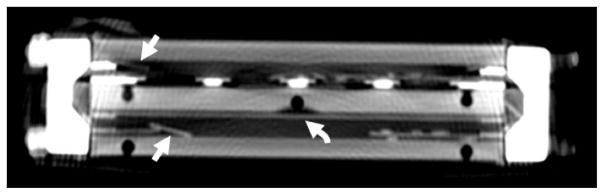
Results: Both linear and exponential models of contrast decay appeared to be reasonable approximations, yielding similar results for contrast diffusion during a single pass through the cartridge. There was no measurable difference in contrast diffusion when comparing 1 mL/min and 20 mL/min flow rates. Fluoroscopy allowed a gross qualitative assessment of flow within the device, and revealed flow inhomogeneity within the corner of the cartridge opposite the blood inlet port. MRI and HR-QCT were both severely limited due to the paramagnetic properties and high atomic number of the target material, respectively. During testing, we encountered several causes of device malfunction, including leak formation, trapped gas, and contrast-mediated nanopore clogging. We illustrate the imaging manifestations of each.
Conclusions: Despite the inherent challenges in imaging a predominantly metallic device, some modalities show potential in the non-invasive assessment of a novel compact hemodialyzer. The approaches described here could potentially be translated to device evaluation in the implanted setting.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
