Significance of intraprostatic architecture and regrowth velocity for considering discontinuation of dutasteride after combination therapy with an alpha blocker: a prospective, pilot study.
{"title":"Significance of intraprostatic architecture and regrowth velocity for considering discontinuation of dutasteride after combination therapy with an alpha blocker: a prospective, pilot study.","authors":"Tetsuya Shindo, Kohei Hashimoto, Takashi Shimizu, Naoki Itoh, Naoya Masumori","doi":"10.4111/kju.2015.56.4.305","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We conducted a prospective single-center study to evaluate the possibility of discontinuation of dutasteride after combination therapy with an alpha blocker for benign prostatic hyperplasia (BPH).</p><p><strong>Materials and methods: </strong>We prospectively treated BPH patients with an alpha blocker and dutasteride (0.5 mg/d). Patients who had been treated with alpha blockers against BPH for more than 2 months were eligible, and 20 patients were included in the study. After 6 months of combination therapy, dutasteride was discontinued. Patients were followed for 12 months after cessation. Prostate volume, intraprostatic architecture determined by transrectal ultrasound, peak urinary flow rate, postvoid residual urine volume, and the serum prostate-specific antigen level were evaluated every 6 months, and the International Prostate Symptom Score and overactive bladder symptom score (OABSS) every 3 months. Patients were allowed to restart dutasteride during the follow-up period according to their desire.</p><p><strong>Results: </strong>Twelve patients (12/20, 60%) restarted the combination therapy from 6 to 12 months into the follow-up period. For patients who restarted dutasteride, the prostate volume and OABSS had increased and worsened after discontinuation, respectively. A visible transition zone with a clear border on transrectal ultrasound at baseline and regrowth of the prostate after discontinuation of dutasteride were risk factors for restarting the therapy (Mann-Whitney U test: p=0.008, p=0.017).</p><p><strong>Conclusions: </strong>Prostatic enlargement after discontinuation of dutasteride differs among patients. Rapid regrowth of the prostate leads to deterioration of storage symptoms and a tendency to restart dutasteride. Baseline intraprostatic architecture may be a predictive factor for whether the patient is a good candidate for discontinuation.</p>","PeriodicalId":17819,"journal":{"name":"Korean Journal of Urology","volume":"56 4","pages":"305-9"},"PeriodicalIF":0.0000,"publicationDate":"2015-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4111/kju.2015.56.4.305","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4111/kju.2015.56.4.305","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/3/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: We conducted a prospective single-center study to evaluate the possibility of discontinuation of dutasteride after combination therapy with an alpha blocker for benign prostatic hyperplasia (BPH).
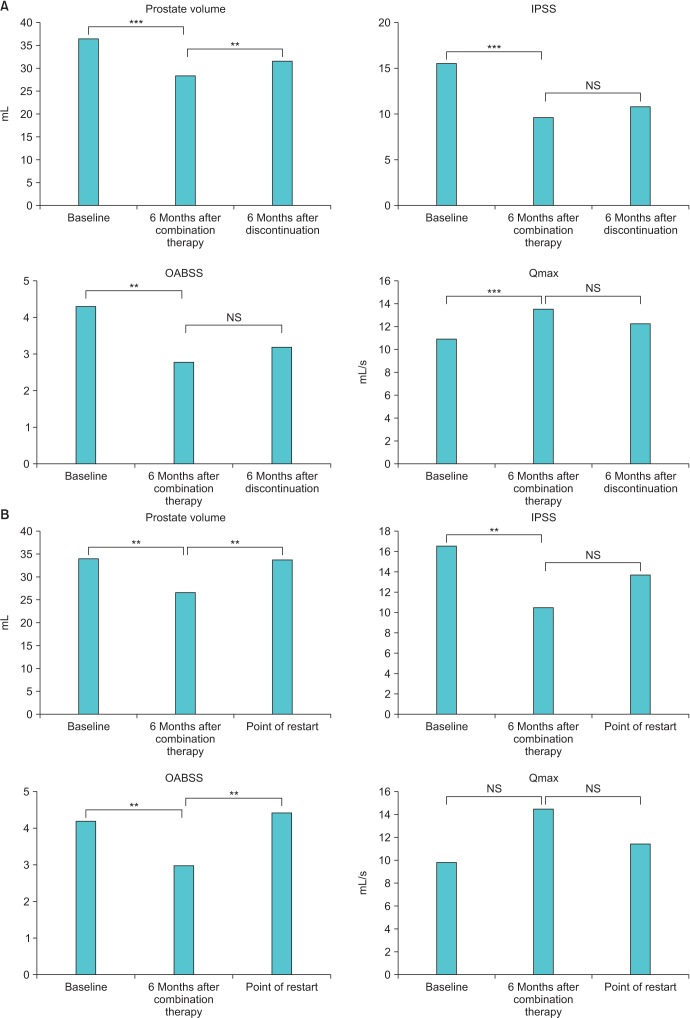
Materials and methods: We prospectively treated BPH patients with an alpha blocker and dutasteride (0.5 mg/d). Patients who had been treated with alpha blockers against BPH for more than 2 months were eligible, and 20 patients were included in the study. After 6 months of combination therapy, dutasteride was discontinued. Patients were followed for 12 months after cessation. Prostate volume, intraprostatic architecture determined by transrectal ultrasound, peak urinary flow rate, postvoid residual urine volume, and the serum prostate-specific antigen level were evaluated every 6 months, and the International Prostate Symptom Score and overactive bladder symptom score (OABSS) every 3 months. Patients were allowed to restart dutasteride during the follow-up period according to their desire.
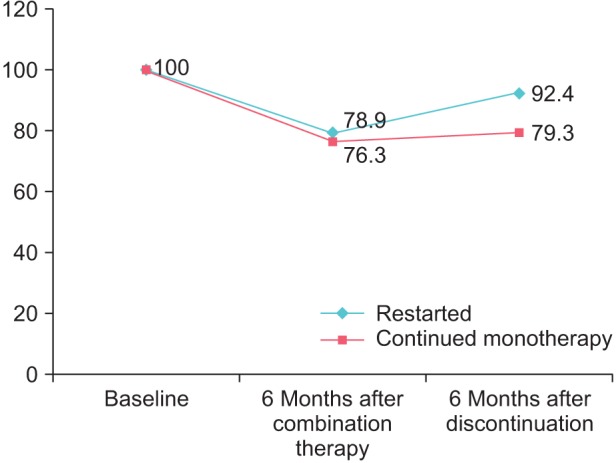
Results: Twelve patients (12/20, 60%) restarted the combination therapy from 6 to 12 months into the follow-up period. For patients who restarted dutasteride, the prostate volume and OABSS had increased and worsened after discontinuation, respectively. A visible transition zone with a clear border on transrectal ultrasound at baseline and regrowth of the prostate after discontinuation of dutasteride were risk factors for restarting the therapy (Mann-Whitney U test: p=0.008, p=0.017).
Conclusions: Prostatic enlargement after discontinuation of dutasteride differs among patients. Rapid regrowth of the prostate leads to deterioration of storage symptoms and a tendency to restart dutasteride. Baseline intraprostatic architecture may be a predictive factor for whether the patient is a good candidate for discontinuation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
