Ji Sung Shim, Hoon Choi, Tae Il Noh, Jong Hyun Tae, Sung Goo Yoon, Seok Ho Kang, Jae Hyun Bae, Hong Seok Park, Jae Young Park
{"title":"The clinical significance of a second transurethral resection for T1 high-grade bladder cancer: Results of a prospective study.","authors":"Ji Sung Shim, Hoon Choi, Tae Il Noh, Jong Hyun Tae, Sung Goo Yoon, Seok Ho Kang, Jae Hyun Bae, Hong Seok Park, Jae Young Park","doi":"10.4111/kju.2015.56.6.429","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study was designed to estimate the value of a second transurethral resection of bladder tumor (TURBT) procedure in patients with initially diagnosed T1 high-grade bladder cancer.</p><p><strong>Materials and methods: </strong>Between August 2009 and January 2013, a total of 29 patients with T1 high-grade bladder cancer prospectively underwent a second TURBT procedure. Evaluation included the presence of previously undetected residual tumor, changes to histopathological staging or grading, and tumor location. Recurrence-free and progression-free survival curves were generated to compare the prognosis between the groups with and without residual lesions by use of the Kaplan-Meier method.</p><p><strong>Results: </strong>Of 29 patients, 22 patients (75.9%) had residual disease after the second TURBT. Staging was as follows: no tumor, 7 (24.1%); Ta, 5 (17.2%); T1, 6 (20.7%); Tis, 6 (20.7%); Ta+Tis, 1 (3.4%); T1+Tis, 1 (3.4%); and ≥T2, 3 (10.3%). The muscle layer was included in the surgical specimen after the initial TURBT in 24 patients (82.7%). In three patients whose cancer was upstaged to pT2 after the second TURBT, the initial surgical specimen contained the muscle layer. In the group with residual lesions, the 3-year recurrence-free survival and 3-year progression-free survival rates were 50% and 66.9%, respectively, whereas these rates were 68.6% and 68.6%, respectively, in the group without residual lesions. This difference was not statistically significant.</p><p><strong>Conclusions: </strong>Initial TURBT does not seem to be enough to control T1 high-grade bladder cancer. Therefore, a routine second TURBT procedure should be recommended in patients with T1 high-grade bladder cancer to accomplish adequate tumor resection and to identify patients who may need to undergo prompt cystectomy.</p>","PeriodicalId":17819,"journal":{"name":"Korean Journal of Urology","volume":"56 6","pages":"429-34"},"PeriodicalIF":0.0000,"publicationDate":"2015-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4111/kju.2015.56.6.429","citationCount":"14","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4111/kju.2015.56.6.429","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/5/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 14
Abstract
Purpose: This study was designed to estimate the value of a second transurethral resection of bladder tumor (TURBT) procedure in patients with initially diagnosed T1 high-grade bladder cancer.
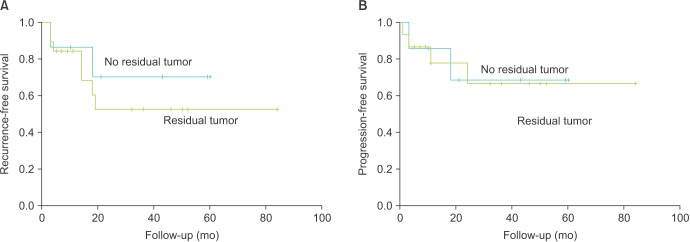
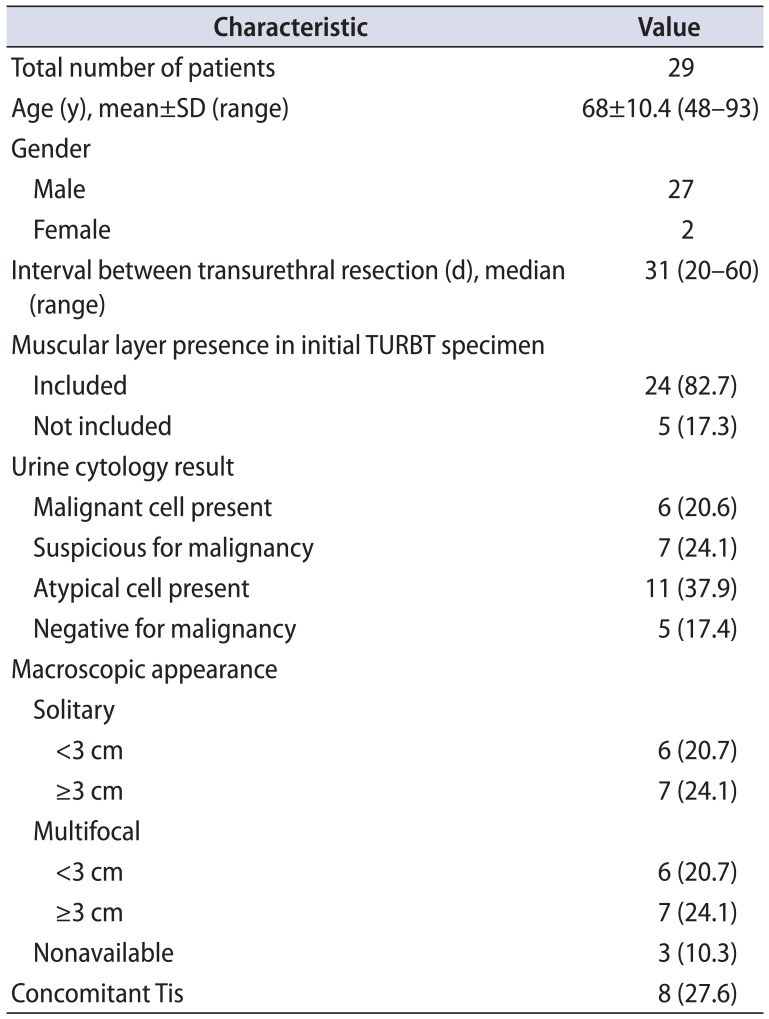
Materials and methods: Between August 2009 and January 2013, a total of 29 patients with T1 high-grade bladder cancer prospectively underwent a second TURBT procedure. Evaluation included the presence of previously undetected residual tumor, changes to histopathological staging or grading, and tumor location. Recurrence-free and progression-free survival curves were generated to compare the prognosis between the groups with and without residual lesions by use of the Kaplan-Meier method.
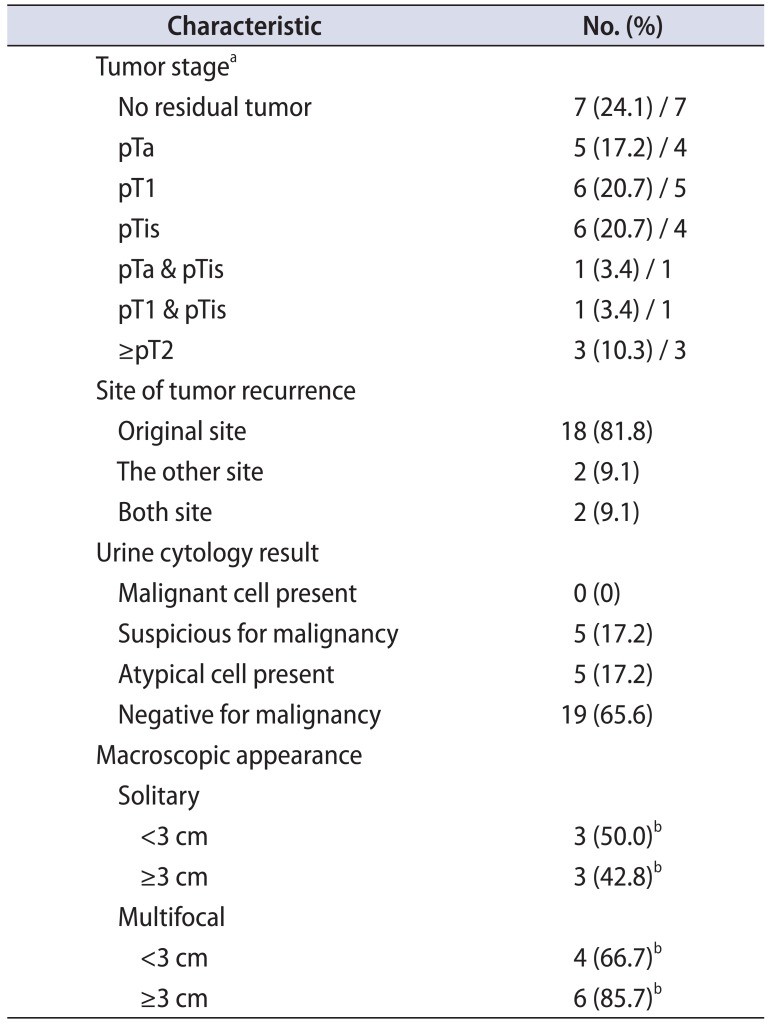
Results: Of 29 patients, 22 patients (75.9%) had residual disease after the second TURBT. Staging was as follows: no tumor, 7 (24.1%); Ta, 5 (17.2%); T1, 6 (20.7%); Tis, 6 (20.7%); Ta+Tis, 1 (3.4%); T1+Tis, 1 (3.4%); and ≥T2, 3 (10.3%). The muscle layer was included in the surgical specimen after the initial TURBT in 24 patients (82.7%). In three patients whose cancer was upstaged to pT2 after the second TURBT, the initial surgical specimen contained the muscle layer. In the group with residual lesions, the 3-year recurrence-free survival and 3-year progression-free survival rates were 50% and 66.9%, respectively, whereas these rates were 68.6% and 68.6%, respectively, in the group without residual lesions. This difference was not statistically significant.
Conclusions: Initial TURBT does not seem to be enough to control T1 high-grade bladder cancer. Therefore, a routine second TURBT procedure should be recommended in patients with T1 high-grade bladder cancer to accomplish adequate tumor resection and to identify patients who may need to undergo prompt cystectomy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
