{"title":"Experience with partial cholecystectomy in severe cholecystitis.","authors":"Whanbong Lee","doi":"10.14701/kjhbps.2013.17.4.171","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Partial cholecystectomy (PC) is often an inevitable operative procedure when Calot triangle is severely inflamed and fibrosed with conglomerated structures. We reviewed our clinical outcomes of PC to compare its feasibility with conventional total cholecystectomy (TC), especially for its possible application to laparoscopic procedure.</p><p><strong>Methods: </strong>From Aug. 2000 to July 2008, 20 cases of PC by laparotomy were performed, including converted cases during laparoscopic cholecystectomy. Sixty-eight cases of TC by open method during the same period were compared in a mean follow-up period of 108 months.</p><p><strong>Results: </strong>Bile fistula was observed in 3 cases of PC; one case needed endoscopic biliary stent for management and a second case showed fistula that closed by supportive care in 2 months. The last patient died from peritonitis. No bile fistula was observed in PC. Morbidities were found in 9 cases of PC (45%) and in 11 cases of TC (16.2%). Bile fistula (n=3) and wound infection (n=3) were prominent in the PC group, and wound infection (n=7) in the TC group. Reoperations were necessary for 5 (25.0%) and 4 (5.9%) patients from PC and TC, respectively. Mortality occurred in 2 (2/10 10%) and 4 cases (4/68 5.9%) of PC and TC, respectively. Two mortalities in each group resulted from direct extension of cholecystitis.</p><p><strong>Conclusions: </strong>Considering the higher risks of complications and mortality, PC should be avoided as long as possible, and patients should always be informed of its clinical outcomes postoperatively. Further elaboration of a safer operative plan should be sought.</p>","PeriodicalId":91136,"journal":{"name":"Korean journal of hepato-biliary-pancreatic surgery","volume":"17 4","pages":"171-5"},"PeriodicalIF":0.0000,"publicationDate":"2013-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.14701/kjhbps.2013.17.4.171","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean journal of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/kjhbps.2013.17.4.171","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/11/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Backgrounds/aims: Partial cholecystectomy (PC) is often an inevitable operative procedure when Calot triangle is severely inflamed and fibrosed with conglomerated structures. We reviewed our clinical outcomes of PC to compare its feasibility with conventional total cholecystectomy (TC), especially for its possible application to laparoscopic procedure.
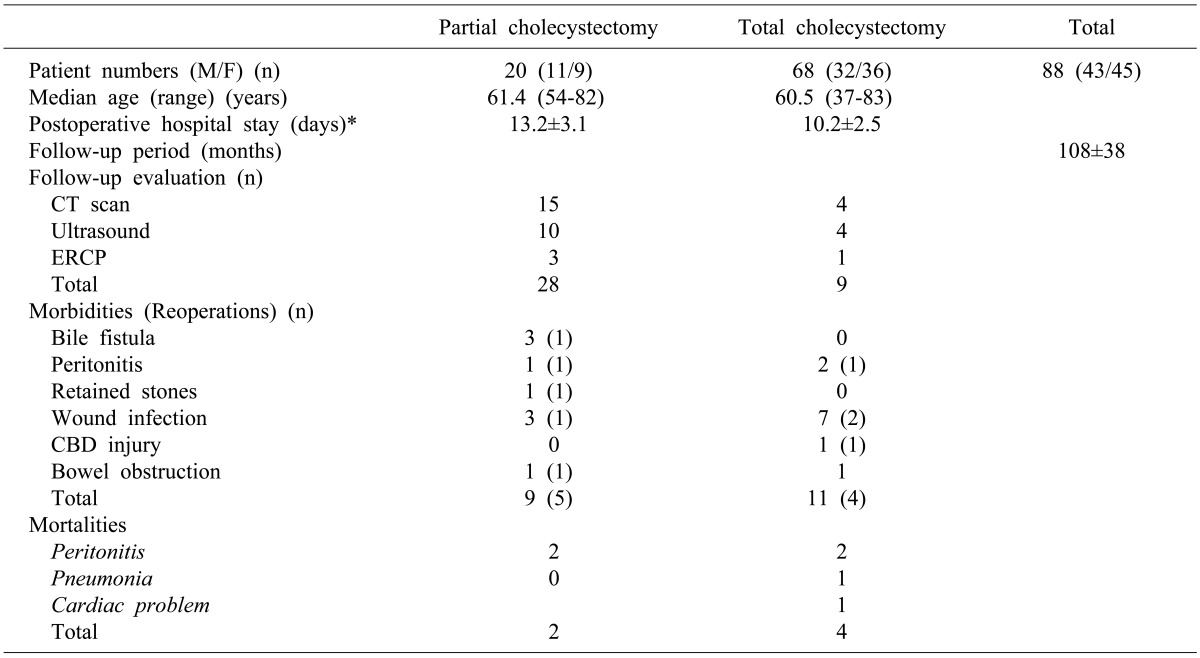
Methods: From Aug. 2000 to July 2008, 20 cases of PC by laparotomy were performed, including converted cases during laparoscopic cholecystectomy. Sixty-eight cases of TC by open method during the same period were compared in a mean follow-up period of 108 months.
Results: Bile fistula was observed in 3 cases of PC; one case needed endoscopic biliary stent for management and a second case showed fistula that closed by supportive care in 2 months. The last patient died from peritonitis. No bile fistula was observed in PC. Morbidities were found in 9 cases of PC (45%) and in 11 cases of TC (16.2%). Bile fistula (n=3) and wound infection (n=3) were prominent in the PC group, and wound infection (n=7) in the TC group. Reoperations were necessary for 5 (25.0%) and 4 (5.9%) patients from PC and TC, respectively. Mortality occurred in 2 (2/10 10%) and 4 cases (4/68 5.9%) of PC and TC, respectively. Two mortalities in each group resulted from direct extension of cholecystitis.
Conclusions: Considering the higher risks of complications and mortality, PC should be avoided as long as possible, and patients should always be informed of its clinical outcomes postoperatively. Further elaboration of a safer operative plan should be sought.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
