Ji Won Kim, Hyoung Keun Park, Hyeong Gon Kim, Dong Yeub Ham, Sung Hyun Paick, Yong Soo Lho, Woo Suk Choi
{"title":"Discordance between location of positive cores in biopsy and location of positive surgical margin following radical prostatectomy.","authors":"Ji Won Kim, Hyoung Keun Park, Hyeong Gon Kim, Dong Yeub Ham, Sung Hyun Paick, Yong Soo Lho, Woo Suk Choi","doi":"10.4111/kju.2015.56.10.710","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We compared location of positive cores in biopsy and location of positive surgical margin (PSM) following radical prostatectomy.</p><p><strong>Materials and methods: </strong>This retrospective analysis included patients who were diagnosed as prostate cancer by standard 12-core transrectal ultrasonography guided prostate biopsy, and who have PSM after radical prostatectomy. After exclusion of number of biopsy cores <12, and lack of biopsy location data, 46 patients with PSM were identified. Locations of PSM in pathologic specimen were reported as 6 difference sites (apex, base and lateral in both sides). Discordance of biopsy result and PSM was defined when no positive cores in biopsy was identified at the location of PSM.</p><p><strong>Results: </strong>Most common location of PSM were right apex (n=21) and left apex (n=15). Multiple PSM was reported in 21 specimens (45.7%). In 32 specimens (69.6%) with PSM, one or more concordant positive biopsy cores were identified, but 14 specimens (28%) had no concordant biopsy cores at PSM location. When discordant rate was separated by locations of PSM, right apex PSM had highest rate of discordant (38%). The discordant group had significantly lower prostate volume and lower number of positive cores in biopsy than concordant group.</p><p><strong>Conclusions: </strong>This study showed that one fourth of PSM occurred at location where tumor was not detected at biopsy and that apex PSM had highest rate of discordant. Careful dissection to avoid PSM should be performed in every location, including where tumor was not identified in biopsy.</p>","PeriodicalId":17819,"journal":{"name":"Korean Journal of Urology","volume":"56 10","pages":"710-6"},"PeriodicalIF":0.0000,"publicationDate":"2015-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4111/kju.2015.56.10.710","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4111/kju.2015.56.10.710","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/10/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Purpose: We compared location of positive cores in biopsy and location of positive surgical margin (PSM) following radical prostatectomy.
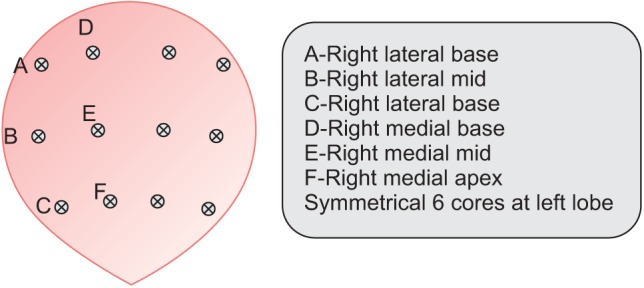
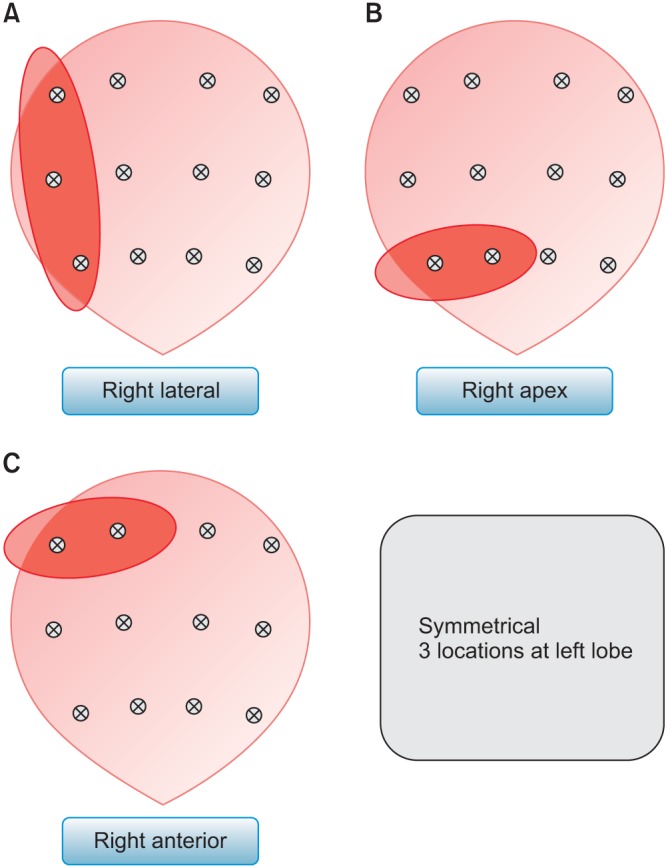
Materials and methods: This retrospective analysis included patients who were diagnosed as prostate cancer by standard 12-core transrectal ultrasonography guided prostate biopsy, and who have PSM after radical prostatectomy. After exclusion of number of biopsy cores <12, and lack of biopsy location data, 46 patients with PSM were identified. Locations of PSM in pathologic specimen were reported as 6 difference sites (apex, base and lateral in both sides). Discordance of biopsy result and PSM was defined when no positive cores in biopsy was identified at the location of PSM.
Results: Most common location of PSM were right apex (n=21) and left apex (n=15). Multiple PSM was reported in 21 specimens (45.7%). In 32 specimens (69.6%) with PSM, one or more concordant positive biopsy cores were identified, but 14 specimens (28%) had no concordant biopsy cores at PSM location. When discordant rate was separated by locations of PSM, right apex PSM had highest rate of discordant (38%). The discordant group had significantly lower prostate volume and lower number of positive cores in biopsy than concordant group.
Conclusions: This study showed that one fourth of PSM occurred at location where tumor was not detected at biopsy and that apex PSM had highest rate of discordant. Careful dissection to avoid PSM should be performed in every location, including where tumor was not identified in biopsy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
