The CECARI Study: Everolimus (Certican®) Initiation and Calcineurin Inhibitor Withdrawal in Maintenance Heart Transplant Recipients with Renal Insufficiency: A Multicenter, Randomized Trial.
Jan Van Keer, David Derthoo, Olivier Van Caenegem, Michel De Pauw, Eric Nellessen, Nathalie Duerinckx, Walter Droogne, Gábor Vörös, Bart Meyns, Ann Belmans, Stefan Janssens, Johan Van Cleemput, Johan Vanhaecke
{"title":"The CECARI Study: Everolimus (Certican®) Initiation and Calcineurin Inhibitor Withdrawal in Maintenance Heart Transplant Recipients with Renal Insufficiency: A Multicenter, Randomized Trial.","authors":"Jan Van Keer, David Derthoo, Olivier Van Caenegem, Michel De Pauw, Eric Nellessen, Nathalie Duerinckx, Walter Droogne, Gábor Vörös, Bart Meyns, Ann Belmans, Stefan Janssens, Johan Van Cleemput, Johan Vanhaecke","doi":"10.1155/2017/6347138","DOIUrl":null,"url":null,"abstract":"<p><p>In this 3-year, open-label, multicenter study, 57 maintenance heart transplant recipients (>1 year after transplant) with renal insufficiency (eGFR 30-60 mL/min/1.73 m<sup>2</sup>) were randomized to start everolimus with CNI withdrawal (<i>N</i> = 29) or continue their current CNI-based immunosuppression (<i>N</i> = 28). The primary endpoint, change in measured glomerular filtration rate (mGFR) from baseline to year 3, did not differ significantly between both groups (+7.0 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, <i>p</i> = 0.18). In the on-treatment analysis, the difference did reach statistical significance (+9.4 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, <i>p</i> = 0.047). The composite safety endpoint of all-cause mortality, major adverse cardiovascular events, or treated acute rejection was not different between groups. Nonfatal adverse events occurred in 96.6% of patients in the everolimus group and 57.1% in the CNI group (<i>p</i> < 0.001). Ten patients (34.5%) in the everolimus group discontinued the study drug during follow-up due to adverse events. The poor adherence to the everolimus therapy might have masked a potential benefit of CNI withdrawal on renal function.</p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2017 ","pages":"6347138"},"PeriodicalIF":2.2000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2017/6347138","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2017/6347138","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/2/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 7
Abstract
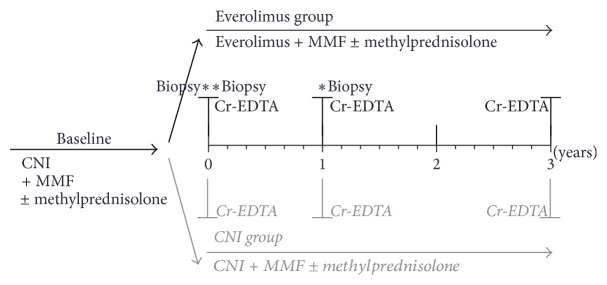
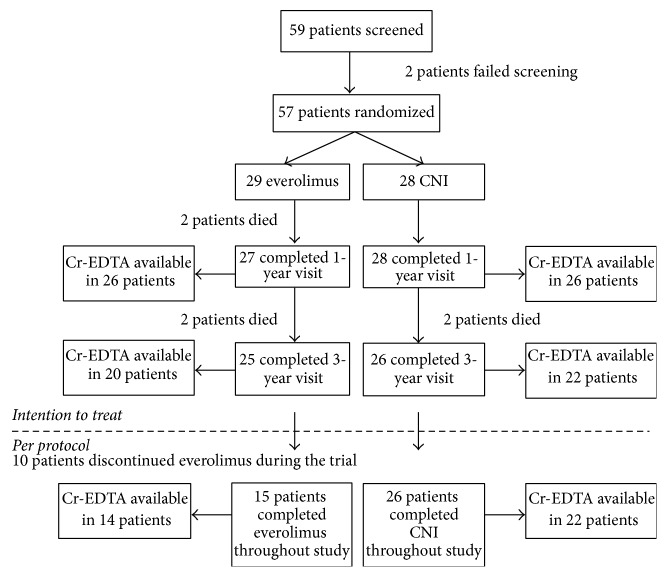
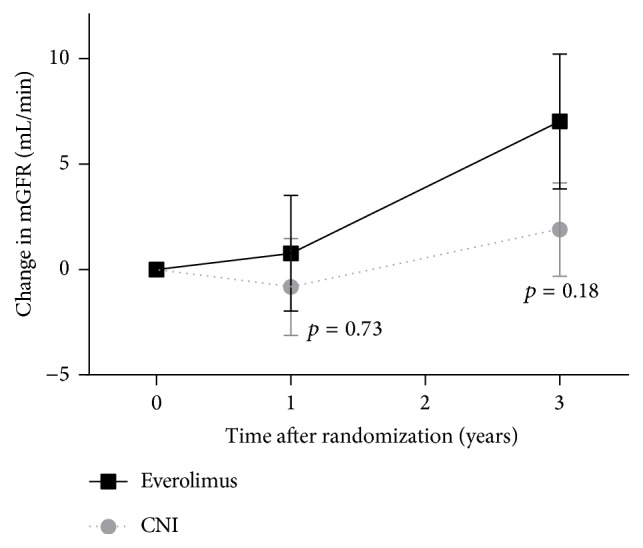
In this 3-year, open-label, multicenter study, 57 maintenance heart transplant recipients (>1 year after transplant) with renal insufficiency (eGFR 30-60 mL/min/1.73 m2) were randomized to start everolimus with CNI withdrawal (N = 29) or continue their current CNI-based immunosuppression (N = 28). The primary endpoint, change in measured glomerular filtration rate (mGFR) from baseline to year 3, did not differ significantly between both groups (+7.0 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, p = 0.18). In the on-treatment analysis, the difference did reach statistical significance (+9.4 mL/min in the everolimus group versus +1.9 mL/min in the CNI group, p = 0.047). The composite safety endpoint of all-cause mortality, major adverse cardiovascular events, or treated acute rejection was not different between groups. Nonfatal adverse events occurred in 96.6% of patients in the everolimus group and 57.1% in the CNI group (p < 0.001). Ten patients (34.5%) in the everolimus group discontinued the study drug during follow-up due to adverse events. The poor adherence to the everolimus therapy might have masked a potential benefit of CNI withdrawal on renal function.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
