Narasa Madam, Wassim Mosleh, Natdanai Punnanithinont, Andres Carmona-Rubio, Zaid H Said, Umesh C Sharma
{"title":"Pulmonary Arterial Enlargement is Associated With Acute Chest Pain in Patients Without Obstructive Coronary Artery Disease.","authors":"Narasa Madam, Wassim Mosleh, Natdanai Punnanithinont, Andres Carmona-Rubio, Zaid H Said, Umesh C Sharma","doi":"10.1177/1179548418758021","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulmonary hypertension (PH) is an underdiagnosed cause for chest pain in patients without significant coronary artery disease (CAD). Studies showed that enlarged pulmonary arterial (PA) and right ventricular chamber sizes correlate with the severity of PH. Therefore, we studied the association between chest pain, right ventricular dimensions (RVDs), and PA size on coronary coronary tomographic angiography (CCTA).</p><p><strong>Methods: </strong>The CCTA of 87 patients presenting with chest pain without evidence of obstructive CAD was examined. The PA diameter (PAD), right atrial dimension (RAD), and RVD were measured. A comparative control cohort included 31 patients who presented without cardiopulmonary complaints and underwent thoracic CT. The risk for obstructive sleep apnea (OSA) was assessed using STOP-BANG questionnaires.</p><p><strong>Results: </strong>Patients with chest pain without obstructive CAD showed markedly dilated right atrial and ventricular chambers compared with standard parameters (right atrium: 48 ± 6.4 mm; right ventricle long axis: 61 ± 9.5 mm). When comparing chest pain vs non-chest pain group, respectively, the mean PAD measured 25.92 ± 0.43 mm vs 22.89 ± 0.38 mm (<i>P</i> < .001), RAD2 measured 40.1423 ± 0.7108 mm vs 34.8800 ± 1.0245 mm (<i>P</i> = .0048), and RVD2 measured 31.7729 ± 0.7299 mm vs 27.6379 ± 1.6178 mm (<i>P</i> = .034). Chest pain was associated with higher PAD (odds ratio [OR]: 11.11, <i>P</i> < .05) after adjusting for age, sex, body mass index, history of hypertension, hyperlipidemia, congestive heart failure, chronic obstructive pulmonary disease, OSA, and smoking. The chest pain group had a mean STOP-BANG score of 3.9 ± 1.8 in all patients, and 3.62 ± 0.20 in patients without known history of OSA, representing an elevated risk index for the disease.</p><p><strong>Conclusions: </strong>In patients presenting with chest pain without obstructive CAD on CCTA, there is a strong association between the presence of chest pain and enlarged PAD. They also represent a high-risk group for OSA.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"12 ","pages":"1179548418758021"},"PeriodicalIF":0.9000,"publicationDate":"2018-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179548418758021","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179548418758021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Pulmonary hypertension (PH) is an underdiagnosed cause for chest pain in patients without significant coronary artery disease (CAD). Studies showed that enlarged pulmonary arterial (PA) and right ventricular chamber sizes correlate with the severity of PH. Therefore, we studied the association between chest pain, right ventricular dimensions (RVDs), and PA size on coronary coronary tomographic angiography (CCTA).
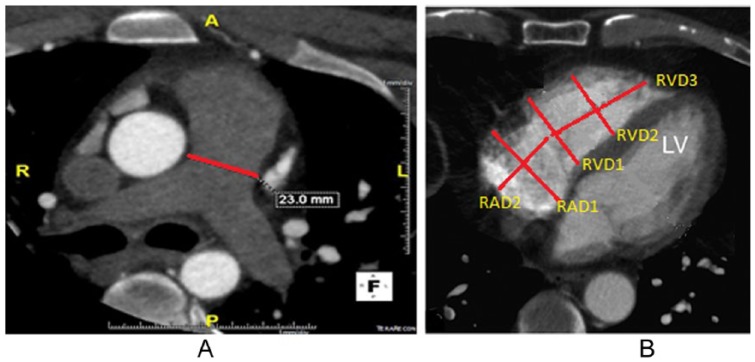
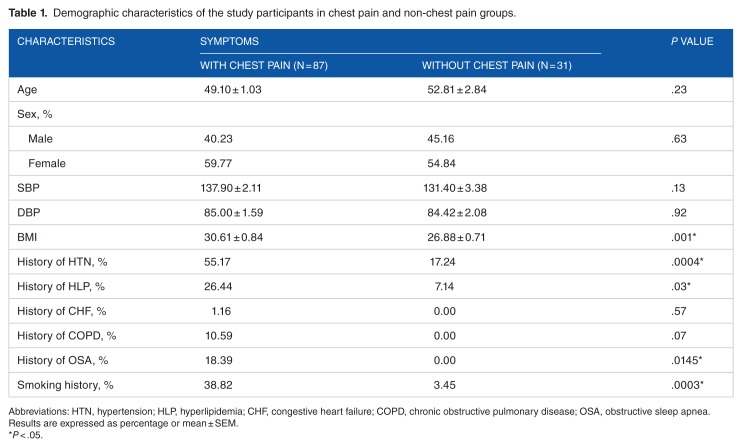
Methods: The CCTA of 87 patients presenting with chest pain without evidence of obstructive CAD was examined. The PA diameter (PAD), right atrial dimension (RAD), and RVD were measured. A comparative control cohort included 31 patients who presented without cardiopulmonary complaints and underwent thoracic CT. The risk for obstructive sleep apnea (OSA) was assessed using STOP-BANG questionnaires.
Results: Patients with chest pain without obstructive CAD showed markedly dilated right atrial and ventricular chambers compared with standard parameters (right atrium: 48 ± 6.4 mm; right ventricle long axis: 61 ± 9.5 mm). When comparing chest pain vs non-chest pain group, respectively, the mean PAD measured 25.92 ± 0.43 mm vs 22.89 ± 0.38 mm (P < .001), RAD2 measured 40.1423 ± 0.7108 mm vs 34.8800 ± 1.0245 mm (P = .0048), and RVD2 measured 31.7729 ± 0.7299 mm vs 27.6379 ± 1.6178 mm (P = .034). Chest pain was associated with higher PAD (odds ratio [OR]: 11.11, P < .05) after adjusting for age, sex, body mass index, history of hypertension, hyperlipidemia, congestive heart failure, chronic obstructive pulmonary disease, OSA, and smoking. The chest pain group had a mean STOP-BANG score of 3.9 ± 1.8 in all patients, and 3.62 ± 0.20 in patients without known history of OSA, representing an elevated risk index for the disease.
Conclusions: In patients presenting with chest pain without obstructive CAD on CCTA, there is a strong association between the presence of chest pain and enlarged PAD. They also represent a high-risk group for OSA.
背景:肺动脉高压(PH)是无明显冠状动脉疾病(CAD)患者胸痛的一个未被诊断的原因。研究表明,肺动脉(PA)增大和右心室大小与ph的严重程度相关。因此,我们研究了胸痛、右心室尺寸(RVDs)和冠状动脉断层血管造影(CCTA)中肺动脉大小之间的关系。方法:对87例无阻塞性CAD证据的胸痛患者进行CCTA检查。测量左房直径(PAD)、右房径(RAD)、RVD。对照队列包括31例无心肺疾患并行胸部CT检查的患者。使用STOP-BANG问卷评估阻塞性睡眠呼吸暂停(OSA)的风险。结果:无阻塞性CAD的胸痛患者与标准参数相比,右心房和心室明显扩张(右心房:48±6.4 mm;右心室长轴:61±9.5 mm)。胸痛组与非胸痛组比较,PAD平均为25.92±0.43 mm vs 22.89±0.38 mm (P = 0.0048), RVD2平均为31.7729±0.7299 mm vs 27.6379±1.6178 mm (P = 0.034)。胸痛与较高的PAD相关(比值比[OR]: 11.11, P)结论:在CCTA上无阻塞性CAD的胸痛患者中,胸痛的存在与PAD增大有很强的相关性。他们也是阻塞性睡眠呼吸暂停的高危人群。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
