Seife Yohannes, Nitin Seam, Junfeng Sun, Joel McAlduff, Janet L Thorne, Susanne B Lara, Michael Keller
{"title":"Impact of an Early Warning System Protocol, for Patients Admitted to the Medical Floors with SARS-COV2 Pneumonia, on ICU Admission.","authors":"Seife Yohannes, Nitin Seam, Junfeng Sun, Joel McAlduff, Janet L Thorne, Susanne B Lara, Michael Keller","doi":"10.1177/11795484231156755","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>COVID-19 placed a significant burden on the global healthcare system. Strain in critical care capacity has been associated with increased COVID-19-related ICU mortality. This study evaluates the impact of an early warning system and response team implemented on medical floors to safely triage and care for critically ill patients on the floor and preserve ICU capacity.</p><p><strong>Methods: </strong>We conducted a multicenter, retrospective cohort study, comparing outcomes between intervention and control hospitals within a US eight-hospital urban network. Patients hospitalized with COVID-19 pneumonia between April 13<sup>th</sup>, 2020 and June 19<sup>th</sup>, 2020 were included in the study, which was a time of a regional surge of COVID-19 admissions. An automated, electronic early warning protocol to identify patients with moderate-severe hypoxemia on the medical floors and implement early interventions was implemented at one of the eight hospitals (\"the intervention hospital\").</p><p><strong>Results: </strong>Among 1024 patients, 403 (39%) were admitted to the intervention hospital and 621 (61%) were admitted to one of the control hospitals. Adjusted for potential confounders, patients at the intervention hospital were less likely to be admitted to the ICU (HR = 0.73, 95% CI 0.53, 1.000, <i>P</i> = .0499) compared to the control hospitals. Patients admitted from the floors to the ICU at the intervention hospital had shorter ICU stay (HR for ICU discharge: 1.74; 95% CI 1.21, 2.51, <i>P</i> = .003). There was no significant difference between intervention and control hospitals in need for mechanical ventilation (OR = 0.93; 95% CI 0.38, 2.31; <i>P</i> = .88) or hospital mortality (OR = 0.79; 95% CI 0.52, 1.18; <i>P</i> = .25).</p><p><strong>Conclusion: </strong>A protocol to conserve ICU beds by implementing an early warning system with a dedicated response team to manage respiratory distress on the floors reduced ICU admission and was not associated with worse outcomes compared to hospitals that managed similar levels of respiratory distress in the ICU.</p>","PeriodicalId":44269,"journal":{"name":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","volume":"17 ","pages":"11795484231156755"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/67/10.1177_11795484231156755.PMC10034308.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Circulatory Respiratory and Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795484231156755","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: COVID-19 placed a significant burden on the global healthcare system. Strain in critical care capacity has been associated with increased COVID-19-related ICU mortality. This study evaluates the impact of an early warning system and response team implemented on medical floors to safely triage and care for critically ill patients on the floor and preserve ICU capacity.
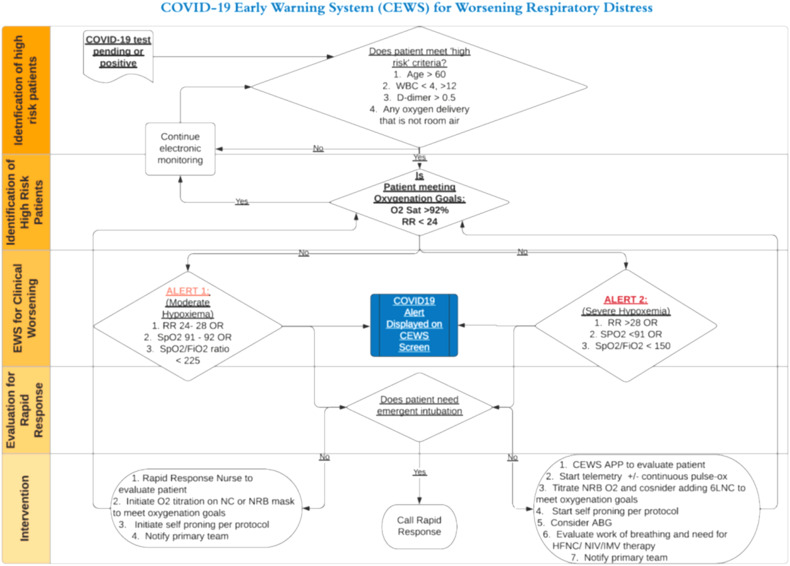
Methods: We conducted a multicenter, retrospective cohort study, comparing outcomes between intervention and control hospitals within a US eight-hospital urban network. Patients hospitalized with COVID-19 pneumonia between April 13th, 2020 and June 19th, 2020 were included in the study, which was a time of a regional surge of COVID-19 admissions. An automated, electronic early warning protocol to identify patients with moderate-severe hypoxemia on the medical floors and implement early interventions was implemented at one of the eight hospitals ("the intervention hospital").
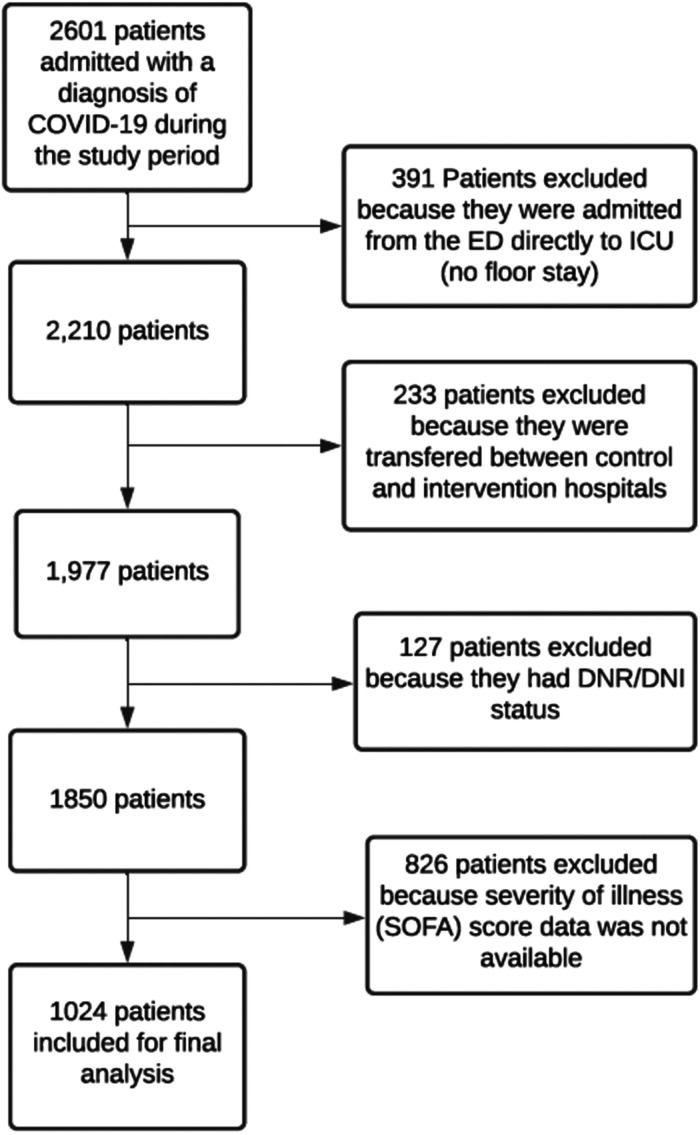
Results: Among 1024 patients, 403 (39%) were admitted to the intervention hospital and 621 (61%) were admitted to one of the control hospitals. Adjusted for potential confounders, patients at the intervention hospital were less likely to be admitted to the ICU (HR = 0.73, 95% CI 0.53, 1.000, P = .0499) compared to the control hospitals. Patients admitted from the floors to the ICU at the intervention hospital had shorter ICU stay (HR for ICU discharge: 1.74; 95% CI 1.21, 2.51, P = .003). There was no significant difference between intervention and control hospitals in need for mechanical ventilation (OR = 0.93; 95% CI 0.38, 2.31; P = .88) or hospital mortality (OR = 0.79; 95% CI 0.52, 1.18; P = .25).
Conclusion: A protocol to conserve ICU beds by implementing an early warning system with a dedicated response team to manage respiratory distress on the floors reduced ICU admission and was not associated with worse outcomes compared to hospitals that managed similar levels of respiratory distress in the ICU.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
