Mahvish Muzaffar, Helen M Johnson, Nasreen A Vohra, Darla Liles, Jan H Wong
{"title":"The Impact of Locoregional Therapy in Nonmetastatic Inflammatory Breast Cancer: A Population-Based Study.","authors":"Mahvish Muzaffar, Helen M Johnson, Nasreen A Vohra, Darla Liles, Jan H Wong","doi":"10.1155/2018/6438635","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Inflammatory breast cancer (IBC) is a rare but most aggressive breast cancer subtype. The impact of locoregional therapy on survival in IBC is controversial.</p><p><strong>Methods: </strong>Patients with nonmetastatic IBC between 1988 and 2013 were identified in the Surveillance, Epidemiology, and End Results (SEER) registry.</p><p><strong>Results: </strong>We identified 7,304 female patients with nonmetastatic inflammatory breast cancer (IBC) who underwent primary tumor surgery. Most patients underwent total mastectomy with only 409 (5.6%) undergoing a partial mastectomy. In addition, 4,559 (62.4%) were also treated with radiation therapy. The patients who underwent mastectomy had better survival compared to partial mastectomy (49% versus 43%, <i>p</i> = 0.003). The addition of radiation therapy was also associated with improved 5-year survival (55% versus 40%, <i>p</i> < 0.001). Multivariate analysis showed that black race HR (1.22, 95% CI 1.18-1.35), ER negative status (HR 1.22, 95% CI 1.16-1.28), and higher grade (HR 1.14, 95% CI 1.07-1.20) were associated with poor outcome. Cox proportional hazards model showed that total mastectomy (HR 0.75, 95% CI 0.65-0.85) and radiation (HR 0.64, 95% CI 0.61-0.69) were associated with improved survival.</p><p><strong>Conclusions: </strong>Optimal locoregional therapy for women with nonmetastatic IBC continues to be mastectomy and radiation therapy. These data reinforce the prevailing treatment algorithm for nonmetastatic IBC.</p>","PeriodicalId":46159,"journal":{"name":"International Journal of Breast Cancer","volume":"2018 ","pages":"6438635"},"PeriodicalIF":3.0000,"publicationDate":"2018-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/6438635","citationCount":"14","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Breast Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/6438635","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 14
Abstract
Background: Inflammatory breast cancer (IBC) is a rare but most aggressive breast cancer subtype. The impact of locoregional therapy on survival in IBC is controversial.
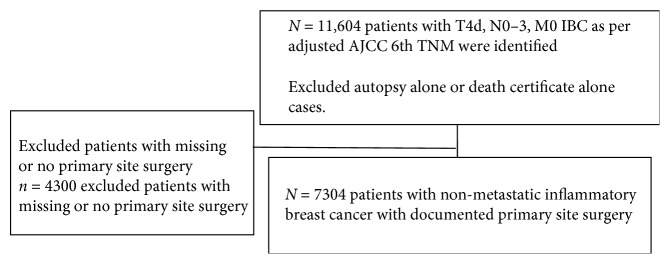
Methods: Patients with nonmetastatic IBC between 1988 and 2013 were identified in the Surveillance, Epidemiology, and End Results (SEER) registry.
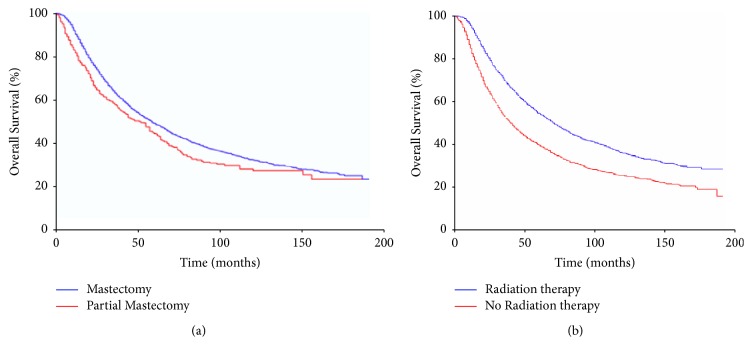
Results: We identified 7,304 female patients with nonmetastatic inflammatory breast cancer (IBC) who underwent primary tumor surgery. Most patients underwent total mastectomy with only 409 (5.6%) undergoing a partial mastectomy. In addition, 4,559 (62.4%) were also treated with radiation therapy. The patients who underwent mastectomy had better survival compared to partial mastectomy (49% versus 43%, p = 0.003). The addition of radiation therapy was also associated with improved 5-year survival (55% versus 40%, p < 0.001). Multivariate analysis showed that black race HR (1.22, 95% CI 1.18-1.35), ER negative status (HR 1.22, 95% CI 1.16-1.28), and higher grade (HR 1.14, 95% CI 1.07-1.20) were associated with poor outcome. Cox proportional hazards model showed that total mastectomy (HR 0.75, 95% CI 0.65-0.85) and radiation (HR 0.64, 95% CI 0.61-0.69) were associated with improved survival.
Conclusions: Optimal locoregional therapy for women with nonmetastatic IBC continues to be mastectomy and radiation therapy. These data reinforce the prevailing treatment algorithm for nonmetastatic IBC.
背景:炎性乳腺癌(IBC)是一种罕见但最具侵袭性的乳腺癌亚型。局部治疗对IBC患者生存的影响存在争议。方法:1988年至2013年间的非转移性IBC患者在监测、流行病学和最终结果(SEER)登记中被确定。结果:我们确定了7,304例接受原发肿瘤手术的非转移性炎性乳腺癌(IBC)女性患者。大多数患者行全乳切除术,只有409例(5.6%)行部分乳切除术。此外,4559例(62.4%)患者也接受了放射治疗。与部分乳房切除术相比,接受乳房切除术的患者生存率更高(49%对43%,p = 0.003)。放疗的增加也与5年生存率的提高相关(55%对40%,p < 0.001)。多因素分析显示,黑人的HR (1.22, 95% CI 1.18-1.35)、ER阴性状态(HR 1.22, 95% CI 1.16-1.28)和较高的分级(HR 1.14, 95% CI 1.07-1.20)与预后不良相关。Cox比例风险模型显示,全乳切除术(HR 0.75, 95% CI 0.65-0.85)和放疗(HR 0.64, 95% CI 0.61-0.69)与生存率提高相关。结论:非转移性IBC的最佳局部治疗仍然是乳房切除术和放疗。这些数据强化了非转移性IBC的主流治疗算法。
期刊介绍:
International Journal of Breast Cancer is a peer-reviewed, Open Access journal that provides a forum for scientists, clinicians, and health care professionals working in breast cancer research and management. The journal publishes original research articles, review articles, and clinical studies related to molecular pathology, genomics, genetic predisposition, screening and diagnosis, disease markers, drug sensitivity and resistance, as well as novel therapies, with a specific focus on molecular targeted agents and immune therapies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
