{"title":"Sonographic Bedside Quantification of Pleural Effusion Compared to Computed Tomography Volumetry in ICU Patients.","authors":"Ulf Karl-Martin Teichgräber, Judith Hackbarth","doi":"10.1055/a-0747-6416","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To date, the reliability of ultrasound for the quantitative assessment of pleural effusion has been limited. In the following study, an easy and cost-effective bedside ultrasound method was developed and investigated for specific use in the intensive care unit (ICU).</p><p><strong>Methods: </strong>22 patients (median age: 58.5 years, range: 37-88 years, 14 men and 8 women) with a total of 31 pleural effusions were examined in the ICU. The inclusion criterion was complete visualization of the effusion on chest computed tomography (CT). The ultrasound (US) examination was performed less than 6 h after the diagnostic CT scan. The pleural effusion volume was calculated volumetrically from the CT scan data. Within 4.58 +/- 2.87 h after the CT scan, all patients were re-examined with US in the ICU. The fluid crescent's thickness was measured between each intercostal space (ICS) with the patient in a supine position and a 30° inclination of the torso. The US measurements were compared to the calculated CT volumes using regression analysis, resulting in the following formula: V=13.330 x ICS6 (V=volume of the effusion [ml]; ICS6=sonographic measurement of the thickness of the liquid crescent [mm] in the sixth ICS).</p><p><strong>Results: </strong>A significant correlation between the sonographically measured and the CT-calculated volumes was best observed for the sixth ICS (R2=0.589; ICC=0.7469 with p<0.0001 and a 95% CI of 0.5364-0.8705).</p><p><strong>Conclusion: </strong>The sonographic assessment of pleural effusions in a supine position and a 30° inclination of the torso is feasible for the volumetric estimation of pleural effusion. This is especially true for ICU patients with severe primary diseases and orthopnea who are unable to sit upright or lie flat.</p>","PeriodicalId":44852,"journal":{"name":"Ultrasound International Open","volume":"4 4","pages":"E131-E135"},"PeriodicalIF":1.6000,"publicationDate":"2018-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/a-0747-6416","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-0747-6416","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/10/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 13
Abstract
Objectives: To date, the reliability of ultrasound for the quantitative assessment of pleural effusion has been limited. In the following study, an easy and cost-effective bedside ultrasound method was developed and investigated for specific use in the intensive care unit (ICU).
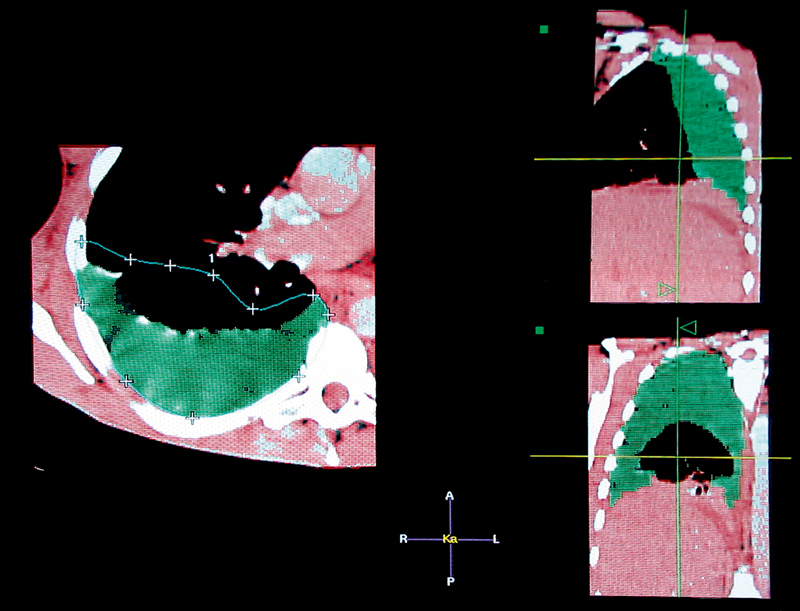
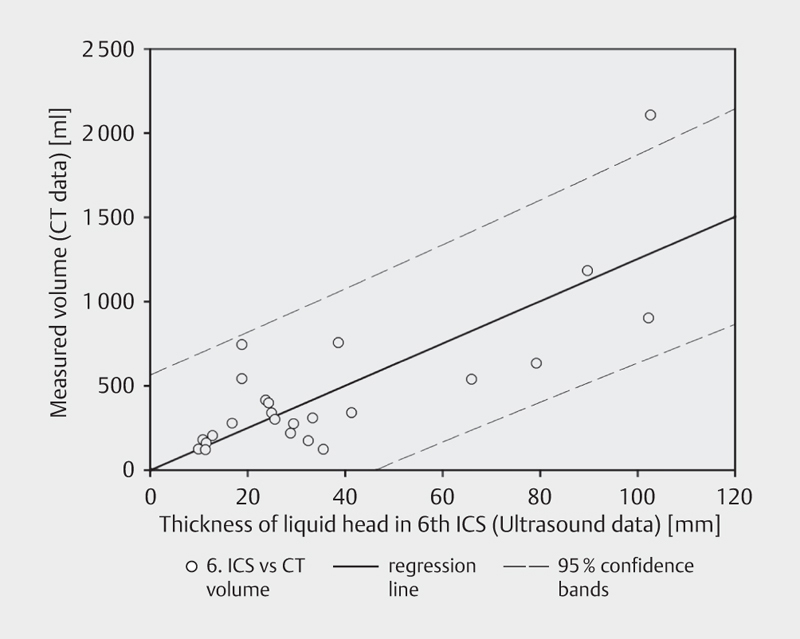
Methods: 22 patients (median age: 58.5 years, range: 37-88 years, 14 men and 8 women) with a total of 31 pleural effusions were examined in the ICU. The inclusion criterion was complete visualization of the effusion on chest computed tomography (CT). The ultrasound (US) examination was performed less than 6 h after the diagnostic CT scan. The pleural effusion volume was calculated volumetrically from the CT scan data. Within 4.58 +/- 2.87 h after the CT scan, all patients were re-examined with US in the ICU. The fluid crescent's thickness was measured between each intercostal space (ICS) with the patient in a supine position and a 30° inclination of the torso. The US measurements were compared to the calculated CT volumes using regression analysis, resulting in the following formula: V=13.330 x ICS6 (V=volume of the effusion [ml]; ICS6=sonographic measurement of the thickness of the liquid crescent [mm] in the sixth ICS).
Results: A significant correlation between the sonographically measured and the CT-calculated volumes was best observed for the sixth ICS (R2=0.589; ICC=0.7469 with p<0.0001 and a 95% CI of 0.5364-0.8705).
Conclusion: The sonographic assessment of pleural effusions in a supine position and a 30° inclination of the torso is feasible for the volumetric estimation of pleural effusion. This is especially true for ICU patients with severe primary diseases and orthopnea who are unable to sit upright or lie flat.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
