Trishul Kapoor, Sean M Wrenn, Peter W Callas, Wasef Abu-Jaish
{"title":"Cost Analysis and Supply Utilization of Laparoscopic Cholecystectomy.","authors":"Trishul Kapoor, Sean M Wrenn, Peter W Callas, Wasef Abu-Jaish","doi":"10.1155/2018/7838103","DOIUrl":null,"url":null,"abstract":"<p><p>Laparoscopic cholecystectomy (LC) is one of the highest volume surgeries performed annually. We hypothesized that there is a statistically significant intradepartmental cost variance with supply utilization variability amongst surgeons of different subspecialty. This study sought to describe laparoscopic cholecystectomy cost of care among three subspecialties of surgeons. This retrospective observational cohort study captured 372 laparoscopic cholecystectomy cases performed between June 2015 and June 2016 by 12 surgeons divided into three subspecialties: 2 in bariatric surgery (BS), 5 in acute care surgery (ACS), and 5 in general surgery (GS). The study utilized a third-party software, Surgical Profitability Compass Procedure Cost Manager and Crimson System (SPCMCS) (The Advisory Board Company, Washington, DC), to stratify case volume, supply cost, case duration, case severity level, and patient length of stay intradepartmentally. Statistical methods included the Kruskal-Wallis test. Average composite supply cost per case was $569 and median supply cost per case was $554. The case volume was 133 (BS), 109 (ACS), and 130 (GS). The median intradepartmental total supply cost was $674.5 (BS), $534 (ACS), and $564 (GS) (P<0.005). ACS and GS presented with a higher standard deviation of cost, $98 (ACS) and $110 (GS) versus $26 (BS). The median case duration was 70 min (BS), 107 min (ACS), and 78 min (GS) (P<0.02). The average patient length of stay was 1.15 (BS), 3.10 (ACS), and 1.17 (GS) (P<0.005). Overall, there was a statistically significant difference in median supply cost (highest in BS; lowest in ACS and GS). However, the higher supply costs may be attenuated by decreased operative time and patient length of stay. Strategies to reduce total supply cost per case include mandating exchange of expensive items, standardization of supply sets, increased price transparency, and education to surgeons.</p>","PeriodicalId":45110,"journal":{"name":"Minimally Invasive Surgery","volume":"2018 ","pages":"7838103"},"PeriodicalIF":1.3000,"publicationDate":"2018-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/7838103","citationCount":"32","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Minimally Invasive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/7838103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 32
Abstract
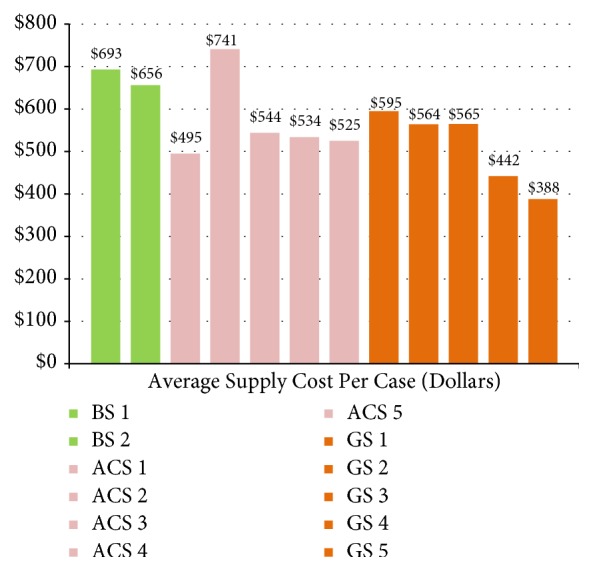
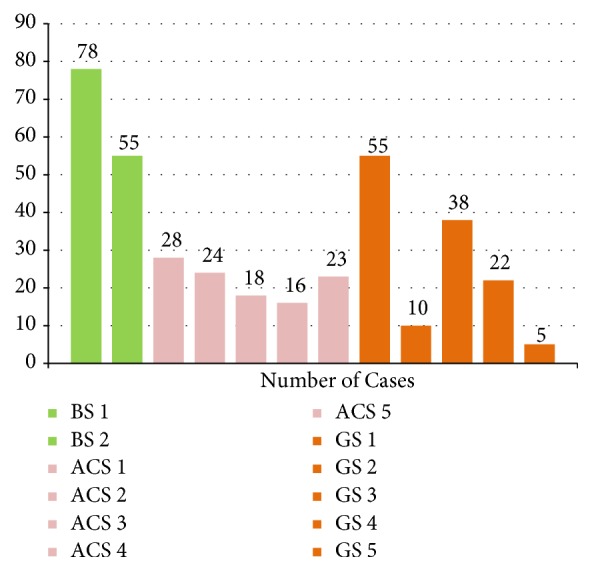
Laparoscopic cholecystectomy (LC) is one of the highest volume surgeries performed annually. We hypothesized that there is a statistically significant intradepartmental cost variance with supply utilization variability amongst surgeons of different subspecialty. This study sought to describe laparoscopic cholecystectomy cost of care among three subspecialties of surgeons. This retrospective observational cohort study captured 372 laparoscopic cholecystectomy cases performed between June 2015 and June 2016 by 12 surgeons divided into three subspecialties: 2 in bariatric surgery (BS), 5 in acute care surgery (ACS), and 5 in general surgery (GS). The study utilized a third-party software, Surgical Profitability Compass Procedure Cost Manager and Crimson System (SPCMCS) (The Advisory Board Company, Washington, DC), to stratify case volume, supply cost, case duration, case severity level, and patient length of stay intradepartmentally. Statistical methods included the Kruskal-Wallis test. Average composite supply cost per case was $569 and median supply cost per case was $554. The case volume was 133 (BS), 109 (ACS), and 130 (GS). The median intradepartmental total supply cost was $674.5 (BS), $534 (ACS), and $564 (GS) (P<0.005). ACS and GS presented with a higher standard deviation of cost, $98 (ACS) and $110 (GS) versus $26 (BS). The median case duration was 70 min (BS), 107 min (ACS), and 78 min (GS) (P<0.02). The average patient length of stay was 1.15 (BS), 3.10 (ACS), and 1.17 (GS) (P<0.005). Overall, there was a statistically significant difference in median supply cost (highest in BS; lowest in ACS and GS). However, the higher supply costs may be attenuated by decreased operative time and patient length of stay. Strategies to reduce total supply cost per case include mandating exchange of expensive items, standardization of supply sets, increased price transparency, and education to surgeons.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
