Gisela Kobelt, Linus Jönsson, Miluse Pavelcova, Eva Kubala Havrdová
{"title":"Real-Life Outcome in Multiple Sclerosis in the Czech Republic.","authors":"Gisela Kobelt, Linus Jönsson, Miluse Pavelcova, Eva Kubala Havrdová","doi":"10.1155/2019/7290285","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cohort studies and registries provide opportunities to estimate long-term outcome in multiple sclerosis.</p><p><strong>Objectives: </strong>To describe changes in disability (EDSS), relapse activity, and health care consumption over the period 2008-2015 by combining two Czech cost-of-illness studies with disease data from the MS Center in Prague.</p><p><strong>Methods: </strong>The combined dataset included 426 patients with a mean observation time of 8.3 years. A Cox proportional hazards model with time-varying covariates for treatment, disease course, and EDSS was applied to estimate the effect of treatment on the risk of progression to EDSS 4 and the risk of relapses. The use of health care resources (hospitalization, consultation, and tests) was compared between the two cross-sectional studies.</p><p><strong>Results: </strong>Total health care costs appeared stable between 2008 and 2015, despite more intense use of disease-modifying treatments in 2015 (52% of patients versus 31% in 2008). 39% of patients starting treatment at EDSS 0-3 in 2008 progressed to EDSS 4 or higher by 2015, while 65% of patients starting at EDSS 0-2 remained stable. The number of relapses was associated with a higher risk of progression. In a marginal structural Cox model of the relapse risk, treatment with natalizumab or fingolimod was associated with a lower risk of relapse (hazard ratio 0.68, p<0.01). Treatment with natalizumab or fingolimod was associated with a lower risk of progression to EDSS 4.</p><p><strong>Conclusion: </strong>Our results link relapses to progression and indicate that the newer treatments have a better effectiveness, despite difficulties caused by small a sample size, administrative rules guiding treatment, and absence of a random comparator group.</p>","PeriodicalId":46096,"journal":{"name":"Multiple Sclerosis International","volume":"2019 ","pages":"7290285"},"PeriodicalIF":2.2000,"publicationDate":"2019-02-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2019/7290285","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Multiple Sclerosis International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/7290285","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Cohort studies and registries provide opportunities to estimate long-term outcome in multiple sclerosis.
Objectives: To describe changes in disability (EDSS), relapse activity, and health care consumption over the period 2008-2015 by combining two Czech cost-of-illness studies with disease data from the MS Center in Prague.
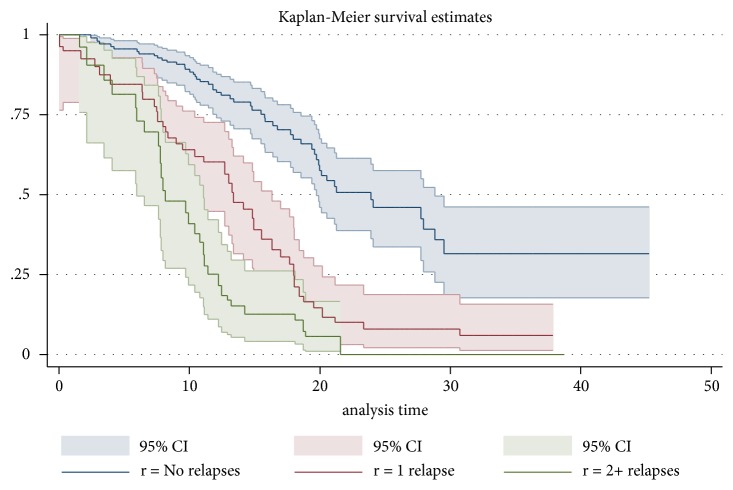
Methods: The combined dataset included 426 patients with a mean observation time of 8.3 years. A Cox proportional hazards model with time-varying covariates for treatment, disease course, and EDSS was applied to estimate the effect of treatment on the risk of progression to EDSS 4 and the risk of relapses. The use of health care resources (hospitalization, consultation, and tests) was compared between the two cross-sectional studies.
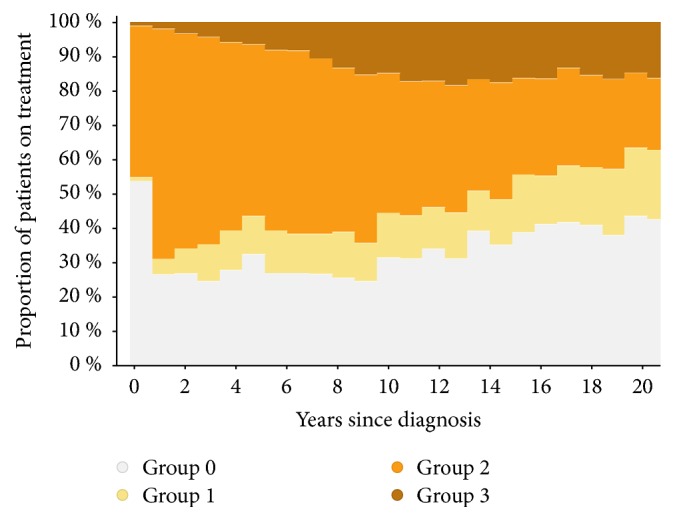
Results: Total health care costs appeared stable between 2008 and 2015, despite more intense use of disease-modifying treatments in 2015 (52% of patients versus 31% in 2008). 39% of patients starting treatment at EDSS 0-3 in 2008 progressed to EDSS 4 or higher by 2015, while 65% of patients starting at EDSS 0-2 remained stable. The number of relapses was associated with a higher risk of progression. In a marginal structural Cox model of the relapse risk, treatment with natalizumab or fingolimod was associated with a lower risk of relapse (hazard ratio 0.68, p<0.01). Treatment with natalizumab or fingolimod was associated with a lower risk of progression to EDSS 4.
Conclusion: Our results link relapses to progression and indicate that the newer treatments have a better effectiveness, despite difficulties caused by small a sample size, administrative rules guiding treatment, and absence of a random comparator group.
期刊介绍:
Multiple Sclerosis International is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies related to all aspects of multiple sclerosis, including clinical neurology, neuroimaging, neuropathology, therapeutics, genetics, neuroimmunology, biomarkers, psychology and neurorehabilitation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
