Christian Eder, Ariane Scheller, Nina Schwab, Björn Dirk Krapohl
{"title":"Hamate's coronal fracture: diagnostic and therapeutic approaches based on a long-term follow-up.","authors":"Christian Eder, Ariane Scheller, Nina Schwab, Björn Dirk Krapohl","doi":"10.3205/iprs000131","DOIUrl":null,"url":null,"abstract":"<p><p>Hamate fractures are commonly divided into hook fractures and body fractures. The coronal fractures as a special form of hamate's body fracture are very rare injuries. Because of unspecific clinical findings and the mostly inconclusive x-ray imaging, these fractures are frequently overseen or misdiagnosed. This leads to further complications like secondary arthritis, persisting pain, and functional deficits in patient's wrist mobility. In our study, a collocation of coronal hamate fractures is analyzed and evaluated with respect to functional outcome after operative treatment and compared to the literature. Furthermore, we compare the strategies for diagnosis and treatment in our clinical center with those presented in the literature. Our standard in the initial diagnostic process is to obtain radiographs in an anterior-posterior, lateral, and 30° oblique view of the wrist. For further diagnosis and preoperative planning, a CT scan of the wrist is obligatory. Due to the high occurrence of comorbidities (especially CMC dislocations) all patients in our cohort obtained operative treatment. In long-term post-operative evaluation, we present the following results: The Manchester-Modified Disability of the Shoulder, Arm and Hand Score (M<sup>2</sup> DASH) imposed with an average of 26.22 points (MD=22/ SD=11.31/MIN=18/MAX=52). None of the re-evaluated patients sorrowed for severe pain in rest. Four patients stated pain (ranging from 3 to 5 on numeric analogue scale) after heavy burden (e.g. boxing, weight lifting). In exploring the range of motion of the operated hand the following results are obtained: dorsal extension: average 83.33° (MD=85°/SD=3.54°/MIN=75°/MAX=85°), flexion: average 77.78° (MD=80°/SD=4.41°/MIN=70°/MAX=80°). Additionally, a performance testing was conducted: fist clenching sign: complete without pain in 100%, pinch grip: complete in 77.78%, opposition digitus manus I-V complete in 66.67%. The conservative treatment is not recommended (especially shown in the here presented \"add\" case with a misdiagnosed fracture). The open approach has its advantages compared to a closed operative procedure and should always be intraoperatively considered as an operative expansion.</p>","PeriodicalId":43347,"journal":{"name":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","volume":"8 ","pages":"Doc05"},"PeriodicalIF":1.5000,"publicationDate":"2019-03-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6459031/pdf/","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/iprs000131","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 8
Abstract
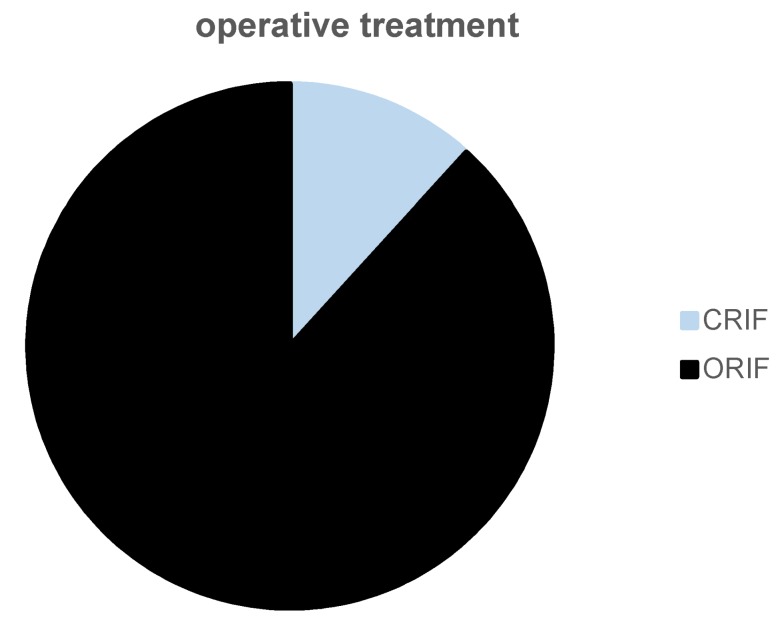
Hamate fractures are commonly divided into hook fractures and body fractures. The coronal fractures as a special form of hamate's body fracture are very rare injuries. Because of unspecific clinical findings and the mostly inconclusive x-ray imaging, these fractures are frequently overseen or misdiagnosed. This leads to further complications like secondary arthritis, persisting pain, and functional deficits in patient's wrist mobility. In our study, a collocation of coronal hamate fractures is analyzed and evaluated with respect to functional outcome after operative treatment and compared to the literature. Furthermore, we compare the strategies for diagnosis and treatment in our clinical center with those presented in the literature. Our standard in the initial diagnostic process is to obtain radiographs in an anterior-posterior, lateral, and 30° oblique view of the wrist. For further diagnosis and preoperative planning, a CT scan of the wrist is obligatory. Due to the high occurrence of comorbidities (especially CMC dislocations) all patients in our cohort obtained operative treatment. In long-term post-operative evaluation, we present the following results: The Manchester-Modified Disability of the Shoulder, Arm and Hand Score (M2 DASH) imposed with an average of 26.22 points (MD=22/ SD=11.31/MIN=18/MAX=52). None of the re-evaluated patients sorrowed for severe pain in rest. Four patients stated pain (ranging from 3 to 5 on numeric analogue scale) after heavy burden (e.g. boxing, weight lifting). In exploring the range of motion of the operated hand the following results are obtained: dorsal extension: average 83.33° (MD=85°/SD=3.54°/MIN=75°/MAX=85°), flexion: average 77.78° (MD=80°/SD=4.41°/MIN=70°/MAX=80°). Additionally, a performance testing was conducted: fist clenching sign: complete without pain in 100%, pinch grip: complete in 77.78%, opposition digitus manus I-V complete in 66.67%. The conservative treatment is not recommended (especially shown in the here presented "add" case with a misdiagnosed fracture). The open approach has its advantages compared to a closed operative procedure and should always be intraoperatively considered as an operative expansion.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
