Estimation of Gastric Volume Before Anesthesia in Term-Pregnant Women Undergoing Elective Cesarean Section, Compared With Non-pregnant or First-Trimester Women Undergoing Minor Gynecological Surgical Procedures.
Oren Gal, Mark Rotshtein, Dan Feldman, Amir Mari, Motti Hallak, Yael Kopelman
{"title":"Estimation of Gastric Volume Before Anesthesia in Term-Pregnant Women Undergoing Elective Cesarean Section, Compared With Non-pregnant or First-Trimester Women Undergoing Minor Gynecological Surgical Procedures.","authors":"Oren Gal, Mark Rotshtein, Dan Feldman, Amir Mari, Motti Hallak, Yael Kopelman","doi":"10.1177/1179562X19828372","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traditionally, intubation of pregnant women has been performed using a rapid sequence induction. This is due to the classical concept that women with more than 18 weeks of pregnancy (mid-second trimester) are always considered to have an increased risk of aspiration due to a number of factors, regardless of the fasting duration. Rapid sequence induction is associated with a higher rate of adverse events.</p><p><strong>Aims: </strong>Our study aimed to illuminate the hypothesis that there is no difference in gastric volume between term-pregnant women and non-pregnant or first-trimester pregnant women who were undergoing minor gynecological surgical procedures. Accordingly, we measured gastric volume and content before anesthesia in term-pregnant women undergoing elective cesarean section, and to compare it with non-pregnant or first-trimester pregnant women who were undergoing minor gynecological surgical procedures.</p><p><strong>Methods: </strong>In this single-center prospective study, the gastric volume and content were assessed by abdominal ultrasound (AUS) just prior to the scheduled procedure. AUS was performed in the sagittal or para-sagittal plain in the upright position and the stomach content was estimated according to the antral circumferential area. Group 1 consisted of 50 term-pregnant women scheduled for cesarean section. Group 2 consisted of 45 non-pregnant or first-trimester pregnant women who were scheduled for minor gynecologic procedure.</p><p><strong>Results: </strong>Despite significant longer fasting time prior to the interventional procedure in the non-pregnant or first-trimester women group, there was no significant difference in gastric volume between term-pregnant and first-trimester pregnant women (3.2 ± 0.97 cm<sup>2</sup> vs 3.2 ± 0.79 cm<sup>2</sup>; <i>P</i> = .97). Gastric volume was small in the two groups.</p><p><strong>Conclusion: </strong>Fasting gastric volume before cesarean section in term-pregnant women is small and is not different than in non-pregnant or first-trimester women undergoing minor gynecologic procedures. Ultrasound estimation of gastric volume is a reliable and easy-to-perform technique which might help in decision-making regarding the airway management prior to induction of anesthesia in pregnant women.</p>","PeriodicalId":90142,"journal":{"name":"Clinical medicine insights. Women's health","volume":"12 ","pages":"1179562X19828372"},"PeriodicalIF":0.0000,"publicationDate":"2019-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4c/47/10.1177_1179562X19828372.PMC6419245.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical medicine insights. Women's health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179562X19828372","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Traditionally, intubation of pregnant women has been performed using a rapid sequence induction. This is due to the classical concept that women with more than 18 weeks of pregnancy (mid-second trimester) are always considered to have an increased risk of aspiration due to a number of factors, regardless of the fasting duration. Rapid sequence induction is associated with a higher rate of adverse events.
Aims: Our study aimed to illuminate the hypothesis that there is no difference in gastric volume between term-pregnant women and non-pregnant or first-trimester pregnant women who were undergoing minor gynecological surgical procedures. Accordingly, we measured gastric volume and content before anesthesia in term-pregnant women undergoing elective cesarean section, and to compare it with non-pregnant or first-trimester pregnant women who were undergoing minor gynecological surgical procedures.
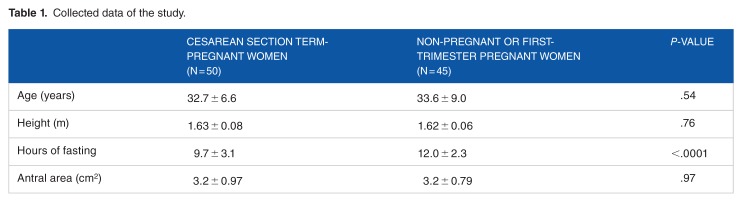
Methods: In this single-center prospective study, the gastric volume and content were assessed by abdominal ultrasound (AUS) just prior to the scheduled procedure. AUS was performed in the sagittal or para-sagittal plain in the upright position and the stomach content was estimated according to the antral circumferential area. Group 1 consisted of 50 term-pregnant women scheduled for cesarean section. Group 2 consisted of 45 non-pregnant or first-trimester pregnant women who were scheduled for minor gynecologic procedure.
Results: Despite significant longer fasting time prior to the interventional procedure in the non-pregnant or first-trimester women group, there was no significant difference in gastric volume between term-pregnant and first-trimester pregnant women (3.2 ± 0.97 cm2 vs 3.2 ± 0.79 cm2; P = .97). Gastric volume was small in the two groups.
Conclusion: Fasting gastric volume before cesarean section in term-pregnant women is small and is not different than in non-pregnant or first-trimester women undergoing minor gynecologic procedures. Ultrasound estimation of gastric volume is a reliable and easy-to-perform technique which might help in decision-making regarding the airway management prior to induction of anesthesia in pregnant women.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
