{"title":"Central pontine myelinolysis during treatment of hyperglycemic hyperosmolar syndrome: a case report.","authors":"Koshi Kusumoto, Nobuyuki Koriyama, Nami Kojima, Maki Ikeda, Yoshihiko Nishio","doi":"10.1186/s40842-020-00111-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Central pontine myelinolysis (CPM) is a non-inflammatory demyelinating lesion of the pons. CPM and extrapontine demyelination (EPM) are together termed osmotic demyelination syndrome (ODS), a known and serious complication of acute correction of hyponatremia. Conversely, hyperglycemic hyperosmolarity syndrome (HHS) develops in patients with type 2 diabetes who still have some insulin secretory ability due to infection, non-compliance with treatment, drugs, and coexisting diseases, and is often accompanied by ketosis. HHS represents a life-threatening endocrine emergency (mortality rate, 10-50%) associated with marked hyperglycemia and severe dehydration. HHS may develop ODS, and some cases have been associated with hypernatremia.</p><p><strong>Case presentation: </strong>The patient was an 87-year-old woman with hyperglycemia, dehydration, malnutrition, and potential thrombus formation during long-term bed rest. HHS was suspected to have developed due to progression of hyperglycemia and dehydration caused by pneumonia. Furthermore, ketoacidosis developed from ketosis and prerenal renal failure associated with circulating hypovolemia shock, which was also associated with disseminated intravascular coagulation. Treatment was started with continuous intravenous injection of fast-acting insulin and low-sodium replacement fluid. In addition, ceftriaxone sodium hydrate, heparin sodium, thrombomodulin α, human serum albumin, and dopamine hydrochloride were administered. Blood glucose, serum sodium, serum osmolality, and general condition (including vital, infection/inflammatory findings, and disseminated intravascular coagulation) improved promptly, but improvements in disturbance of consciousness were poor. Diffusion-weighted imaging of the brain 72 h after starting treatment showed no obvious abnormalities, but high-intensity signals in the midline of the pons became apparent 30 days later, leading to definitive diagnosis of CPM.</p><p><strong>Conclusions: </strong>Fluctuation of osmotic pressure by treatment from hyperosmolarity due to hyperglycemia and hypernatremia in the presence of risk factors such as malnutrition, severe illness, and metabolic disorders may be a cause of CPM onset. When treating HHS with risk factors, the possibility of progression to ODS needs to be kept in mind.</p>","PeriodicalId":56339,"journal":{"name":"Clinical Diabetes and Endocrinology","volume":"6 1","pages":"23"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40842-020-00111-6","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Diabetes and Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40842-020-00111-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
Abstract
Background: Central pontine myelinolysis (CPM) is a non-inflammatory demyelinating lesion of the pons. CPM and extrapontine demyelination (EPM) are together termed osmotic demyelination syndrome (ODS), a known and serious complication of acute correction of hyponatremia. Conversely, hyperglycemic hyperosmolarity syndrome (HHS) develops in patients with type 2 diabetes who still have some insulin secretory ability due to infection, non-compliance with treatment, drugs, and coexisting diseases, and is often accompanied by ketosis. HHS represents a life-threatening endocrine emergency (mortality rate, 10-50%) associated with marked hyperglycemia and severe dehydration. HHS may develop ODS, and some cases have been associated with hypernatremia.
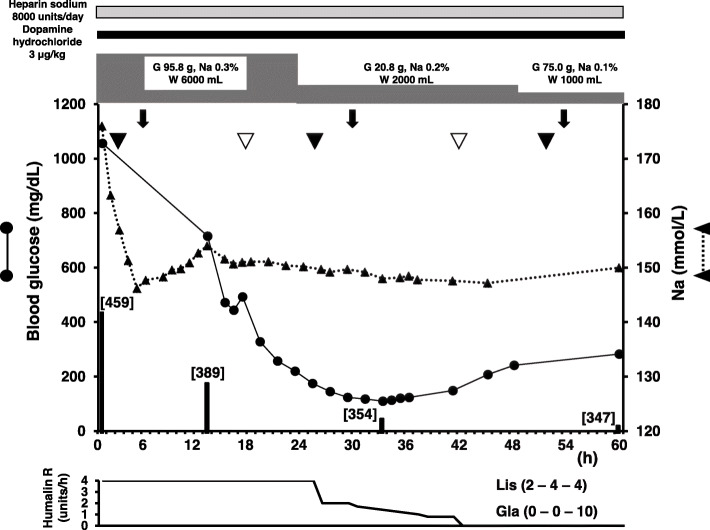
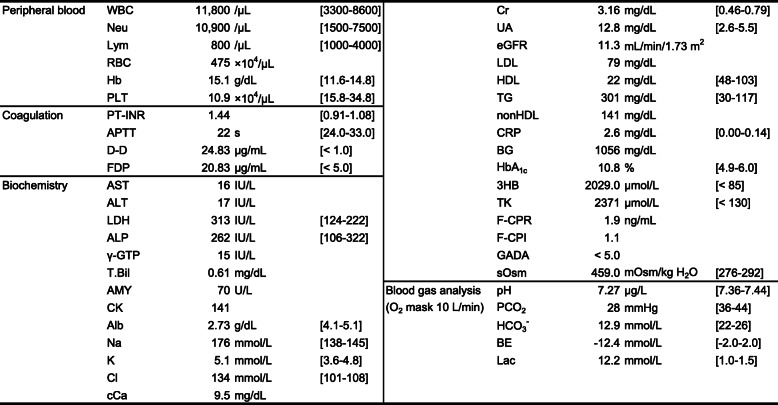
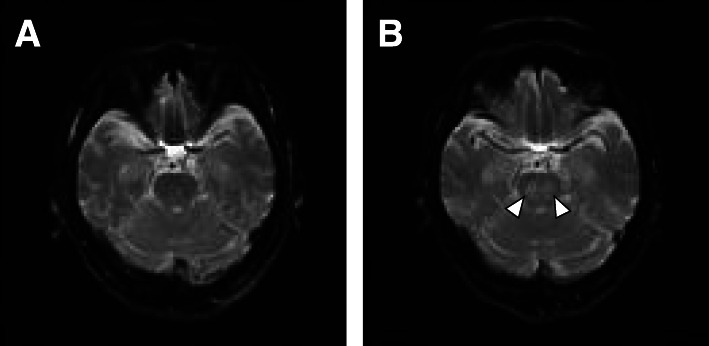
Case presentation: The patient was an 87-year-old woman with hyperglycemia, dehydration, malnutrition, and potential thrombus formation during long-term bed rest. HHS was suspected to have developed due to progression of hyperglycemia and dehydration caused by pneumonia. Furthermore, ketoacidosis developed from ketosis and prerenal renal failure associated with circulating hypovolemia shock, which was also associated with disseminated intravascular coagulation. Treatment was started with continuous intravenous injection of fast-acting insulin and low-sodium replacement fluid. In addition, ceftriaxone sodium hydrate, heparin sodium, thrombomodulin α, human serum albumin, and dopamine hydrochloride were administered. Blood glucose, serum sodium, serum osmolality, and general condition (including vital, infection/inflammatory findings, and disseminated intravascular coagulation) improved promptly, but improvements in disturbance of consciousness were poor. Diffusion-weighted imaging of the brain 72 h after starting treatment showed no obvious abnormalities, but high-intensity signals in the midline of the pons became apparent 30 days later, leading to definitive diagnosis of CPM.
Conclusions: Fluctuation of osmotic pressure by treatment from hyperosmolarity due to hyperglycemia and hypernatremia in the presence of risk factors such as malnutrition, severe illness, and metabolic disorders may be a cause of CPM onset. When treating HHS with risk factors, the possibility of progression to ODS needs to be kept in mind.
期刊介绍:
Clinical Diabetes and Endocrinology is an open access journal publishing within the field of diabetes and endocrine disease. The journal aims to provide a widely available resource for people working within the field of diabetes and endocrinology, in order to improve the care of people affected by these conditions. The audience includes, but is not limited to, physicians, researchers, nurses, nutritionists, pharmacists, podiatrists, psychologists, epidemiologists, exercise physiologists and health care researchers. Research articles include patient-based research (clinical trials, clinical studies, and others), translational research (translation of basic science to clinical practice, translation of clinical practice to policy and others), as well as epidemiology and health care research. Clinical articles include case reports, case seminars, consensus statements, clinical practice guidelines and evidence-based medicine. Only articles considered to contribute new knowledge to the field will be considered for publication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
