{"title":"Maximal Glycemic Difference, the Possible Strongest Glycemic Variability Parameter to Predict Mortality in ICU Patients.","authors":"Thanaphruet Issarawattana, Rungsun Bhurayanontachai","doi":"10.1155/2020/5071509","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This retrospective study aimed to determine the correlation of blood glucose and glycemic variability with mortality and to identify the strongest glycemic variability parameter for predicting mortality in critically ill patients.</p><p><strong>Methods: </strong>A total of 528 patients admitted to the medical intensive care unit were included in this study. Blood glucose levels during the first 24 hours of admission were recorded and calculated to determine the glycemic variability. Significant glycemic variability parameters, including the standard deviation, coefficient of variation, maximal blood glucose difference, and J-index, were subsequently compared between intensive care unit survivors and nonsurvivors. A binary logistic regression was performed to identify independent factors associated with mortality. To determine the strongest glycemic variability parameter to predict mortality, the area under the receiver operating characteristic of each glycemic variability parameter was determined, and a pairwise comparison was performed.</p><p><strong>Results: </strong>Among the 528 patients, 17.8% (96/528) were nonsurvivors. Both survivor and nonsurvivor groups were clinically comparable. However, nonsurvivors had significantly higher median APACHE-II scores (23 [21, 27] vs. 18 [14, 22]; <i>p</i> < 0.01) and a higher mechanical ventilator support rate (97.4% vs. 74.9%; <i>p</i> < 0.01). The mean blood glucose level and significant glycemic variability parameters were higher in nonsurvivors than in survivors. The maximal blood glucose difference yielded a similar power to the coefficient of variation (<i>p</i> = 0.21) but was significantly stronger than the standard deviation (<i>p</i> = 0.005) and J-index (<i>p</i> = 0.006).</p><p><strong>Conclusions: </strong>Glycemic variability was independently associated with intensive care unit mortality. Higher glycemic variability was identified in the nonsurvivor group regardless of preexisting diabetes mellitus. The maximal blood glucose difference and coefficient of variation of the blood glucose were the two strongest parameters for predicting intensive care unit mortality in this study.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2020 ","pages":"5071509"},"PeriodicalIF":1.8000,"publicationDate":"2020-08-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/5071509","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/5071509","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 6
Abstract
Background: This retrospective study aimed to determine the correlation of blood glucose and glycemic variability with mortality and to identify the strongest glycemic variability parameter for predicting mortality in critically ill patients.
Methods: A total of 528 patients admitted to the medical intensive care unit were included in this study. Blood glucose levels during the first 24 hours of admission were recorded and calculated to determine the glycemic variability. Significant glycemic variability parameters, including the standard deviation, coefficient of variation, maximal blood glucose difference, and J-index, were subsequently compared between intensive care unit survivors and nonsurvivors. A binary logistic regression was performed to identify independent factors associated with mortality. To determine the strongest glycemic variability parameter to predict mortality, the area under the receiver operating characteristic of each glycemic variability parameter was determined, and a pairwise comparison was performed.
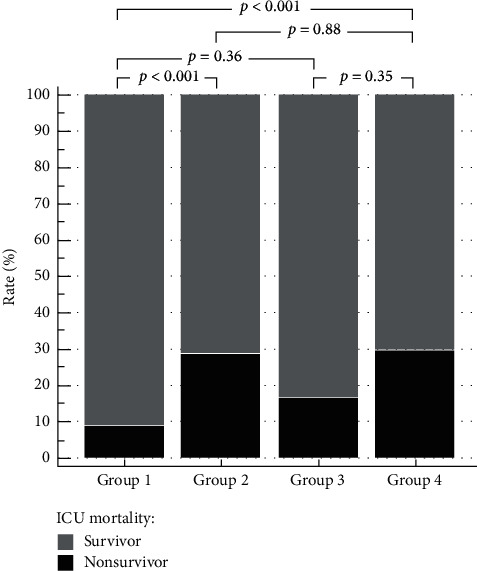
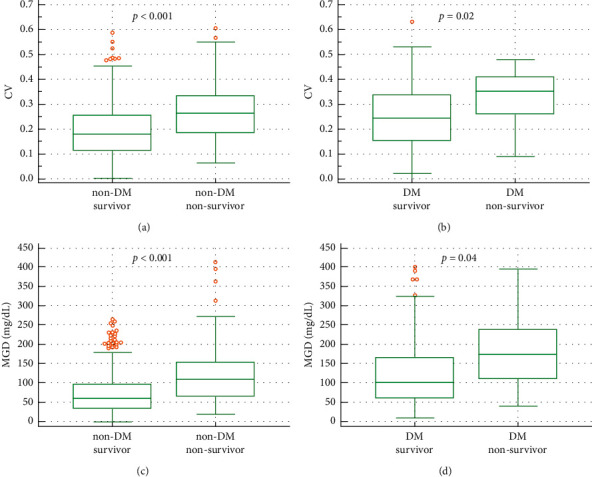
Results: Among the 528 patients, 17.8% (96/528) were nonsurvivors. Both survivor and nonsurvivor groups were clinically comparable. However, nonsurvivors had significantly higher median APACHE-II scores (23 [21, 27] vs. 18 [14, 22]; p < 0.01) and a higher mechanical ventilator support rate (97.4% vs. 74.9%; p < 0.01). The mean blood glucose level and significant glycemic variability parameters were higher in nonsurvivors than in survivors. The maximal blood glucose difference yielded a similar power to the coefficient of variation (p = 0.21) but was significantly stronger than the standard deviation (p = 0.005) and J-index (p = 0.006).
Conclusions: Glycemic variability was independently associated with intensive care unit mortality. Higher glycemic variability was identified in the nonsurvivor group regardless of preexisting diabetes mellitus. The maximal blood glucose difference and coefficient of variation of the blood glucose were the two strongest parameters for predicting intensive care unit mortality in this study.
背景:本回顾性研究旨在确定血糖和血糖变异性与死亡率的相关性,并确定预测危重患者死亡率的最强血糖变异性参数。方法:本研究共纳入528例重症监护病房住院患者。记录并计算入院前24小时的血糖水平,以确定血糖变异性。随后比较重症监护病房幸存者和非幸存者的显著血糖变异性参数,包括标准差、变异系数、最大血糖差和j指数。采用二元逻辑回归来确定与死亡率相关的独立因素。为了确定预测死亡率的最强血糖变异性参数,确定每个血糖变异性参数的受试者操作特征下的面积,并进行两两比较。结果:528例患者中,17.8%(96/528)为非幸存者。生存组和非生存组具有临床可比性。然而,非幸存者的APACHE-II中位评分明显更高(23[21,27]对18 [14,22];p p p = 0.21),但显著强于标准差(p = 0.005)和j指数(p = 0.006)。结论:血糖变异性与重症监护病房死亡率独立相关。无论先前是否存在糖尿病,非幸存者组的血糖变异性都较高。最大血糖差值和血糖变异系数是本研究预测重症监护病房死亡率的两个最重要参数。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
