Alberto Manassero, Matteo Bossolasco, Mattia Carrega, Giuseppe Coletta
{"title":"Postoperative Thoracic Epidural Analgesia: Adverse Events from a Single-Center Series of 3126 Patients.","authors":"Alberto Manassero, Matteo Bossolasco, Mattia Carrega, Giuseppe Coletta","doi":"10.2147/LRA.S272410","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Thoracic epidural analgesia (TEA) has been shown to reduce postsurgical morbidity and mortality; nevertheless, major and minor complications can occur. We report our 10-year experience with TEA and incidence of complications.</p><p><strong>Patients and methods: </strong>Patients received continuous infusion TEA (0.2% ropivacaine and 2 µg ml<sup>-1</sup> fentanyl) to control postoperative pain. Every 8 hours, the acute pain service recorded the analgesia regimen and occurrence of side effects. The initial infusion rate was tapered daily in response to improvement in pain symptoms or occurrence of side effects.</p><p><strong>Results: </strong>A total of 3126 patients received TEA. The median age was 65 years (range, 18-94) and the duration of catheter placement was 3.5 days (range, 2-8). Three major complications were identified (1:1042): two subarachnoid blocks and one epidural abscess which led to permanent sequela (1:3126). Minor complications were hypotension (4.8%), pruritus (4.4%), accidental catheter removal (3.7%), insertion site inflammation (2.5%), motor weakness (2.0%), postoperative nausea and vomiting (1.8%), catheter disconnection (1.9%), catheter occlusion (0.3%), post-dural puncture headache (0.5%), and catheter fragment retention (0.06%), which were the reasons for a 7.4% rate of early discontinuation of epidural analgesia. No occurrence of epidural hematoma, local anesthetic systemic toxicity, and cardiovascular/respiratory depression was recorded.</p><p><strong>Conclusion: </strong>Postoperative TEA is an advanced technique that poses certain difficulties that can subvert its great potential. While serious complications were rare, minor complications occurred more often and affected the postoperative course negatively. A risk/benefit evaluation of each patient should be done before employing the technique.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"13 ","pages":"111-119"},"PeriodicalIF":1.9000,"publicationDate":"2020-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/LRA.S272410","citationCount":"19","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S272410","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 19
Abstract
Purpose: Thoracic epidural analgesia (TEA) has been shown to reduce postsurgical morbidity and mortality; nevertheless, major and minor complications can occur. We report our 10-year experience with TEA and incidence of complications.
Patients and methods: Patients received continuous infusion TEA (0.2% ropivacaine and 2 µg ml-1 fentanyl) to control postoperative pain. Every 8 hours, the acute pain service recorded the analgesia regimen and occurrence of side effects. The initial infusion rate was tapered daily in response to improvement in pain symptoms or occurrence of side effects.
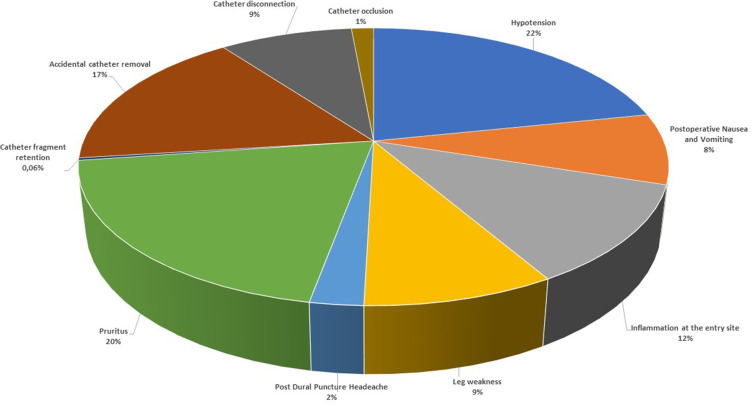
Results: A total of 3126 patients received TEA. The median age was 65 years (range, 18-94) and the duration of catheter placement was 3.5 days (range, 2-8). Three major complications were identified (1:1042): two subarachnoid blocks and one epidural abscess which led to permanent sequela (1:3126). Minor complications were hypotension (4.8%), pruritus (4.4%), accidental catheter removal (3.7%), insertion site inflammation (2.5%), motor weakness (2.0%), postoperative nausea and vomiting (1.8%), catheter disconnection (1.9%), catheter occlusion (0.3%), post-dural puncture headache (0.5%), and catheter fragment retention (0.06%), which were the reasons for a 7.4% rate of early discontinuation of epidural analgesia. No occurrence of epidural hematoma, local anesthetic systemic toxicity, and cardiovascular/respiratory depression was recorded.
Conclusion: Postoperative TEA is an advanced technique that poses certain difficulties that can subvert its great potential. While serious complications were rare, minor complications occurred more often and affected the postoperative course negatively. A risk/benefit evaluation of each patient should be done before employing the technique.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
