Shih Ling Kao, Ying Chen, Yilin Ning, Maudrene Tan, Mark Salloway, Eric Yin Hao Khoo, E Shyong Tai, Chuen Seng Tan
{"title":"Evaluating the effectiveness of a multi-faceted inpatient diabetes management program among hospitalised patients with diabetes mellitus.","authors":"Shih Ling Kao, Ying Chen, Yilin Ning, Maudrene Tan, Mark Salloway, Eric Yin Hao Khoo, E Shyong Tai, Chuen Seng Tan","doi":"10.1186/s40842-020-00107-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetes mellitus (DM) is one of the most common chronic diseases. Individuals with DM are more likely to be hospitalised and stay longer than those without DM. Inpatient hypoglycemia and hyperglycemia, which are associated with adverse outcomes, are common, but can be prevented through hospital quality improvement programs.</p><p><strong>Methods: </strong>We designed a multi-faceted intervention program with the aim of reducing inpatient hypoglycemia and hyperglycemia. This was implemented over seven phases between September 2013 to January 2016, and covered all the non-critical care wards in a tertiary hospital. The program represented a pragmatic approach that leveraged on existing resources and infrastructure within the hospital. We calculated glucometric outcomes in June to August 2016 and compared them with those in June to August 2013 to assess the overall effectiveness of the program. We used regression models with generalised estimating equations to adjust for potential confounders and account for correlations of repeated outcomes within patients and admissions.</p><p><strong>Results: </strong>We observed significant reductions in patient-days affected by hypoglycemia (any glucose reading < 4 mmol/L: OR = 0.71, 95% CI: 0.61 to 0.83, p < 0.001), and hyperglycemia (any glucose reading > 14 mmol/L: OR = 0.84, 95% CI: 0.71 to 0.99, p = 0.041). Similar findings were observed for admission-level hypoglycemia and hyperglycemia. Further analyses suggested that these reductions started to occur four to 6 months post-implementation.</p><p><strong>Conclusions: </strong>Our program was associated with sustained improvements in clinically relevant outcomes. Our described intervention could be feasibly implemented by other secondary and tertiary care hospitals by leveraging on existing infrastructure and work force.</p>","PeriodicalId":56339,"journal":{"name":"Clinical Diabetes and Endocrinology","volume":"6 1","pages":"21"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7643419/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Diabetes and Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40842-020-00107-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Diabetes mellitus (DM) is one of the most common chronic diseases. Individuals with DM are more likely to be hospitalised and stay longer than those without DM. Inpatient hypoglycemia and hyperglycemia, which are associated with adverse outcomes, are common, but can be prevented through hospital quality improvement programs.
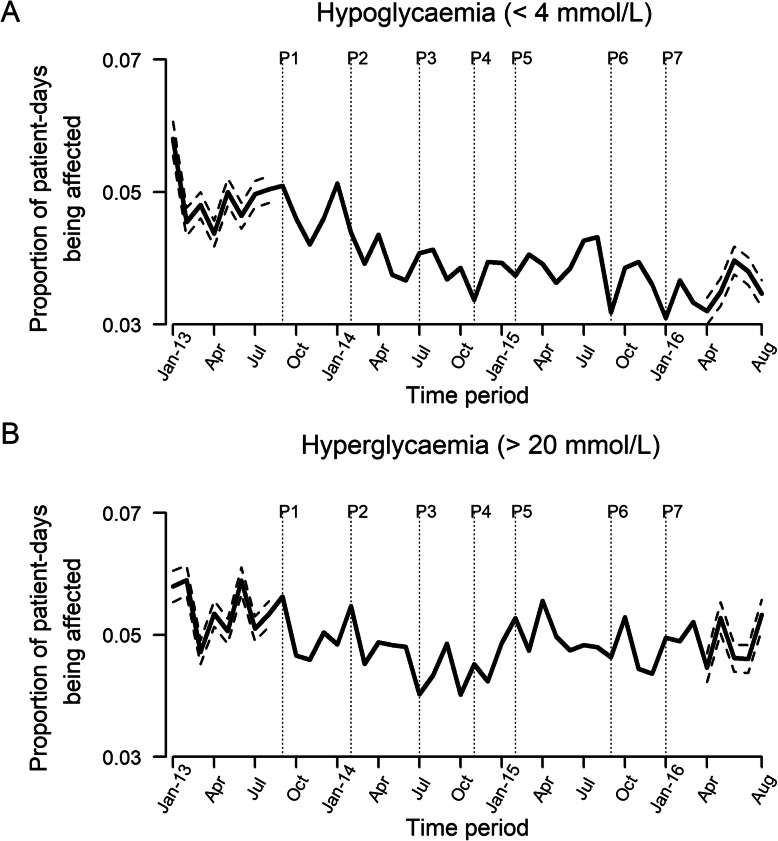
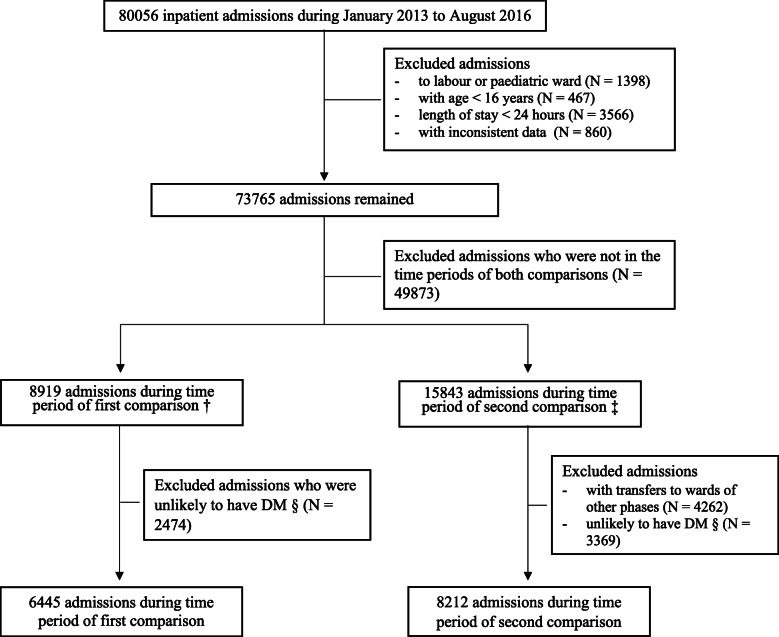
Methods: We designed a multi-faceted intervention program with the aim of reducing inpatient hypoglycemia and hyperglycemia. This was implemented over seven phases between September 2013 to January 2016, and covered all the non-critical care wards in a tertiary hospital. The program represented a pragmatic approach that leveraged on existing resources and infrastructure within the hospital. We calculated glucometric outcomes in June to August 2016 and compared them with those in June to August 2013 to assess the overall effectiveness of the program. We used regression models with generalised estimating equations to adjust for potential confounders and account for correlations of repeated outcomes within patients and admissions.
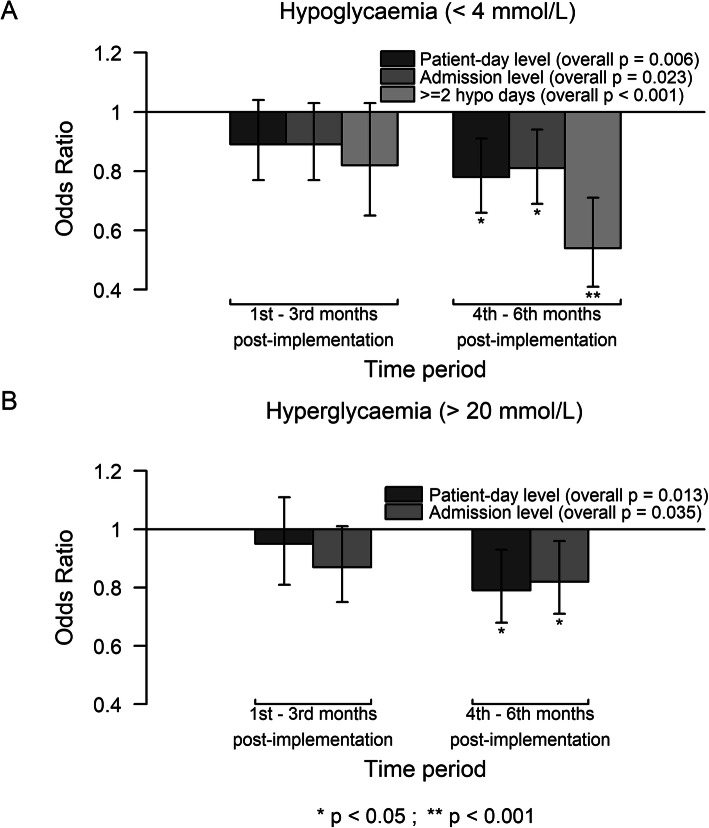
Results: We observed significant reductions in patient-days affected by hypoglycemia (any glucose reading < 4 mmol/L: OR = 0.71, 95% CI: 0.61 to 0.83, p < 0.001), and hyperglycemia (any glucose reading > 14 mmol/L: OR = 0.84, 95% CI: 0.71 to 0.99, p = 0.041). Similar findings were observed for admission-level hypoglycemia and hyperglycemia. Further analyses suggested that these reductions started to occur four to 6 months post-implementation.
Conclusions: Our program was associated with sustained improvements in clinically relevant outcomes. Our described intervention could be feasibly implemented by other secondary and tertiary care hospitals by leveraging on existing infrastructure and work force.
期刊介绍:
Clinical Diabetes and Endocrinology is an open access journal publishing within the field of diabetes and endocrine disease. The journal aims to provide a widely available resource for people working within the field of diabetes and endocrinology, in order to improve the care of people affected by these conditions. The audience includes, but is not limited to, physicians, researchers, nurses, nutritionists, pharmacists, podiatrists, psychologists, epidemiologists, exercise physiologists and health care researchers. Research articles include patient-based research (clinical trials, clinical studies, and others), translational research (translation of basic science to clinical practice, translation of clinical practice to policy and others), as well as epidemiology and health care research. Clinical articles include case reports, case seminars, consensus statements, clinical practice guidelines and evidence-based medicine. Only articles considered to contribute new knowledge to the field will be considered for publication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
