Andreas Sakkas, Sebastian Heil, Steffen Kargus, Martin Rebel, Robert A Mischkowski, Oliver C Thiele
{"title":"Tocilizumab: Another medication related to osteonecrosis of the jaws? A case report and literature review.","authors":"Andreas Sakkas, Sebastian Heil, Steffen Kargus, Martin Rebel, Robert A Mischkowski, Oliver C Thiele","doi":"10.3205/iprs000153","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Medication-related osteonecrosis of the jaw (MRONJ) is a serious complication in patients receiving antiresorptive medication, such as bisphosphonates and denosumab, for different oncologic and non-oncologic diseases. Here, we report a case of MRONJ in a patient treated with tocilizumab, a humanized anti-interleukin-6 receptor antibody that effectively treats moderate to severe rheumatoid arthritis in adults. <b>Case description:</b> A 45-year-old female patient diagnosed with severe rheumatoid arthritis, who had been undergoing intravenous tocilizumab therapy for three years without history of bisphosphonate use, was referred to our department. Four weeks previously, several teeth in the maxilla and mandible were removed under local anesthesia by her dentist. Two weeks after the extractions, she felt pain in both jaws. We diagnosed wound dehiscence and delayed healing of the alveolar bone after the tooth extractions. Digital volume tomography showed persistent dry alveolar sockets. The patient underwent surgical debridement of necrotic bone, and intravenous antibiotics were administered in hospital. Five months later, wound dehiscence reoccurred in the same regions. Histopathological analysis of bone biopsies revealed a diagnosis of MRONJ. Four months later, wound dehiscence occurred in the left maxillary alveolar ridge, and local bone resection was performed under antibiotic treatment. Twenty-four months after the last surgery, wound dehiscence had healed completely without signs of recurrence. <b>Discussion:</b> Osteomyelitis of the jaw in patients treated with tocilizumab has not been reported often. This case confirms the potential role of this interleukin-6 receptor inhibitor in the pathogenesis of MRONJ and shows that patients who receive tocilizumab with MRONJ-like symptoms should be closely monitored. The pathomechanism of MRONJ under tocilizumab therapy remains unclear, so dental practitioners, maxillofacial surgeons, and rheumatologists should look for signs of MRONJ in patients receiving tocilizumab to prevent MRONJ onset.</p>","PeriodicalId":43347,"journal":{"name":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","volume":"10 ","pages":"Doc03"},"PeriodicalIF":1.5000,"publicationDate":"2021-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8054499/pdf/","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS Interdisciplinary Plastic and Reconstructive Surgery DGPW","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/iprs000153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 5
Abstract
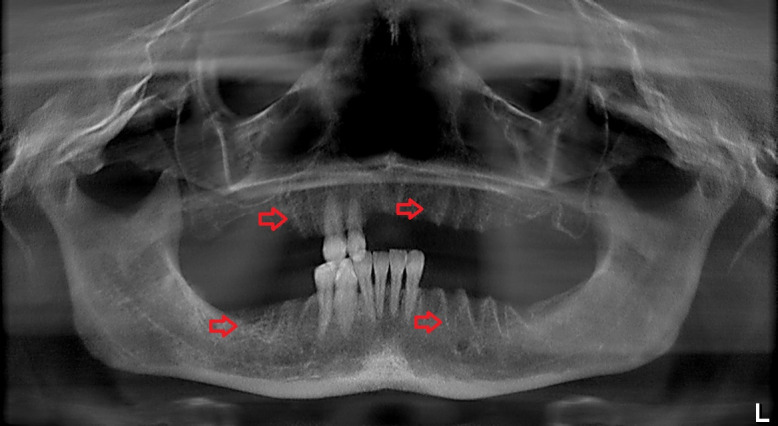
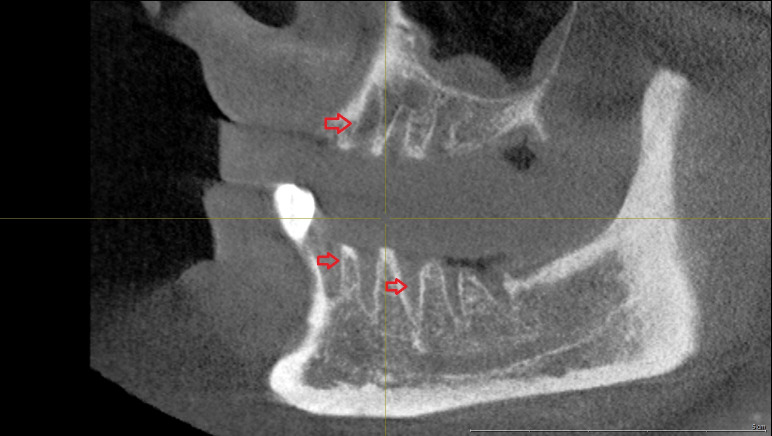
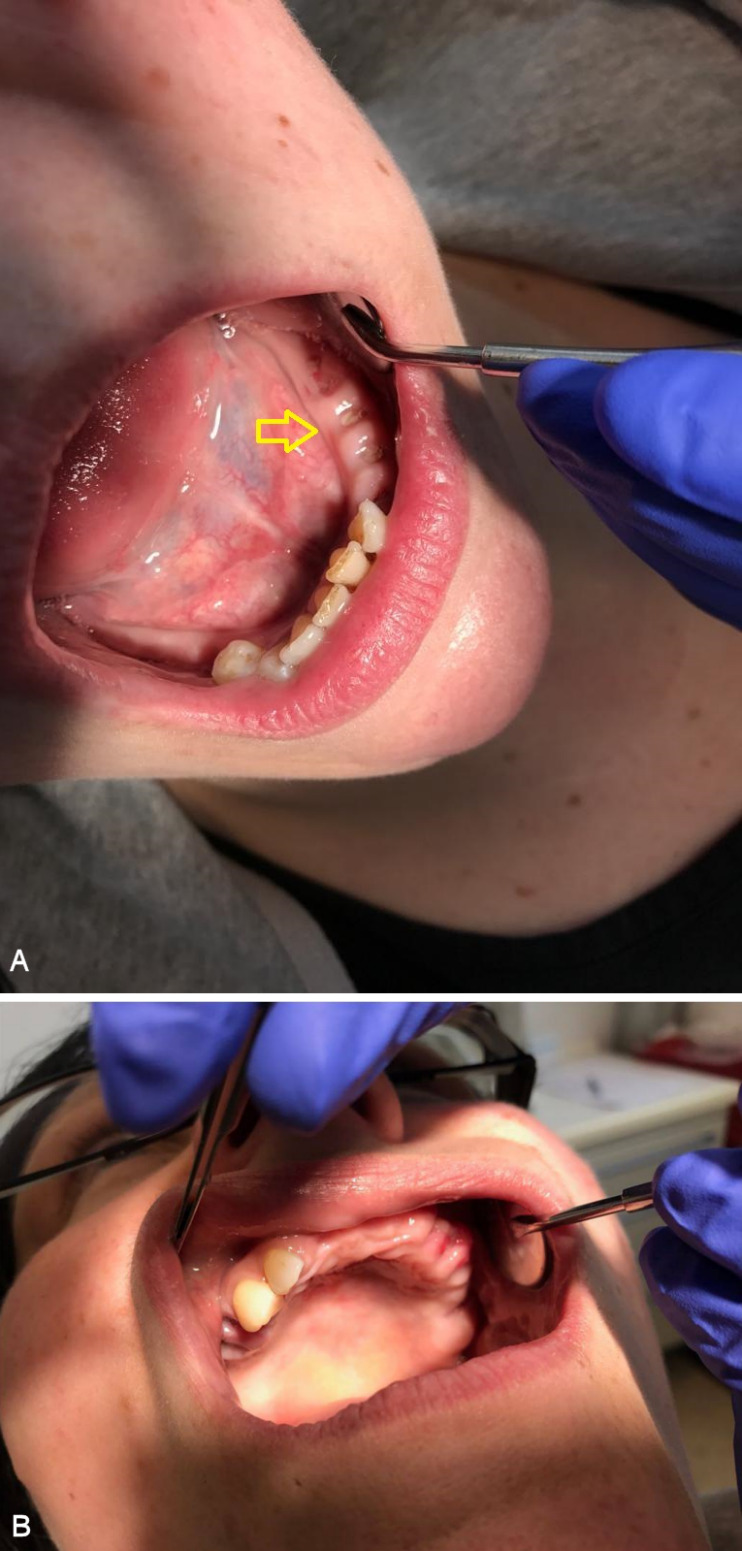
Introduction: Medication-related osteonecrosis of the jaw (MRONJ) is a serious complication in patients receiving antiresorptive medication, such as bisphosphonates and denosumab, for different oncologic and non-oncologic diseases. Here, we report a case of MRONJ in a patient treated with tocilizumab, a humanized anti-interleukin-6 receptor antibody that effectively treats moderate to severe rheumatoid arthritis in adults. Case description: A 45-year-old female patient diagnosed with severe rheumatoid arthritis, who had been undergoing intravenous tocilizumab therapy for three years without history of bisphosphonate use, was referred to our department. Four weeks previously, several teeth in the maxilla and mandible were removed under local anesthesia by her dentist. Two weeks after the extractions, she felt pain in both jaws. We diagnosed wound dehiscence and delayed healing of the alveolar bone after the tooth extractions. Digital volume tomography showed persistent dry alveolar sockets. The patient underwent surgical debridement of necrotic bone, and intravenous antibiotics were administered in hospital. Five months later, wound dehiscence reoccurred in the same regions. Histopathological analysis of bone biopsies revealed a diagnosis of MRONJ. Four months later, wound dehiscence occurred in the left maxillary alveolar ridge, and local bone resection was performed under antibiotic treatment. Twenty-four months after the last surgery, wound dehiscence had healed completely without signs of recurrence. Discussion: Osteomyelitis of the jaw in patients treated with tocilizumab has not been reported often. This case confirms the potential role of this interleukin-6 receptor inhibitor in the pathogenesis of MRONJ and shows that patients who receive tocilizumab with MRONJ-like symptoms should be closely monitored. The pathomechanism of MRONJ under tocilizumab therapy remains unclear, so dental practitioners, maxillofacial surgeons, and rheumatologists should look for signs of MRONJ in patients receiving tocilizumab to prevent MRONJ onset.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
