Effects of Ultrasound-Guided Bilateral Cervical Plexus Block Combined with General Anesthesia in Patients Undergoing Total Parathyroidectomy and Partial Gland Autotransplantation Surgery.
{"title":"Effects of Ultrasound-Guided Bilateral Cervical Plexus Block Combined with General Anesthesia in Patients Undergoing Total Parathyroidectomy and Partial Gland Autotransplantation Surgery.","authors":"Jing Gong, Youxiu Yao, Yanbiao Wang","doi":"10.2147/LRA.S299312","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this study is to evaluate the effect of ultrasound-guided bilateral cervical plexus block on general anesthesia, postoperative analgesia, and surgical outcomes in patients undergoing total parathyroidectomy with autotransplantation.</p><p><strong>Patients and methods: </strong>Forty-eight ASA III-IV patients with hyperparathyroidism secondary to renal failure were included: 24 patients received ultrasound-guided bilateral superficial and deep cervical plexus block combined with general anesthesia (group A), and 24 patients received general anesthesia alone (group B). Postoperative patient-controlled intravenous analgesia was provided with sufentanil 2 μg/kg. The primary outcome is the postoperative pain scores. Secondary outcomes include intraoperative remifentanil dosage, changes in hemodynamics, extubation time, and sufentanil consumption. Surgical outcomes regarding calcium, phosphorus and parathormone values were also noted.</p><p><strong>Results: </strong>The patients in group A required less remifentanil than group B (2.56±0.92mg vs 3.38±0.84mg, <i>P</i>=0.002) and lower VAS scores at 1, 3, 10, 24, and 48h postoperatively (<i>P</i> < 0.001). While the systolic blood pressure in group A patients was significantly greater than that in group B at T3 (immediately after extubation, [138.33±11.36 vs 129.08±17.06 mmHg; <i>P</i>=0.032]), heart rates in group A were lower than in group B at 1 min before induction (T1 [89.46 ± 9.14 vs 96.71±14.19, <i>P</i>=0.042]) and 1 min after intubation (T2 [70.08 ± 5.35 vs 79.25 ± 11.81, <i>P</i>=0.002]). The extubation time in group A was shorter than that in group B (<i>P</i> < 0.001). There was no difference in calcium, phosphorus and parathormone values, nor in sufentanil consumption between the groups.</p><p><strong>Conclusion: </strong>Ultrasound-guided bilateral superficial and deep cervical plexus block combined with general anesthesia for TPTA is an effective strategy to improve anesthesia management and achieve better postoperative analgesia, and has no impact on surgical outcomes.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"14 ","pages":"75-83"},"PeriodicalIF":1.9000,"publicationDate":"2021-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cb/fc/lra-14-75.PMC8079358.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S299312","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The aim of this study is to evaluate the effect of ultrasound-guided bilateral cervical plexus block on general anesthesia, postoperative analgesia, and surgical outcomes in patients undergoing total parathyroidectomy with autotransplantation.
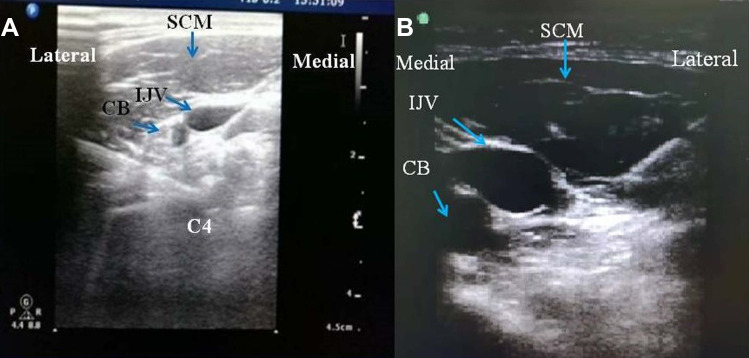
Patients and methods: Forty-eight ASA III-IV patients with hyperparathyroidism secondary to renal failure were included: 24 patients received ultrasound-guided bilateral superficial and deep cervical plexus block combined with general anesthesia (group A), and 24 patients received general anesthesia alone (group B). Postoperative patient-controlled intravenous analgesia was provided with sufentanil 2 μg/kg. The primary outcome is the postoperative pain scores. Secondary outcomes include intraoperative remifentanil dosage, changes in hemodynamics, extubation time, and sufentanil consumption. Surgical outcomes regarding calcium, phosphorus and parathormone values were also noted.
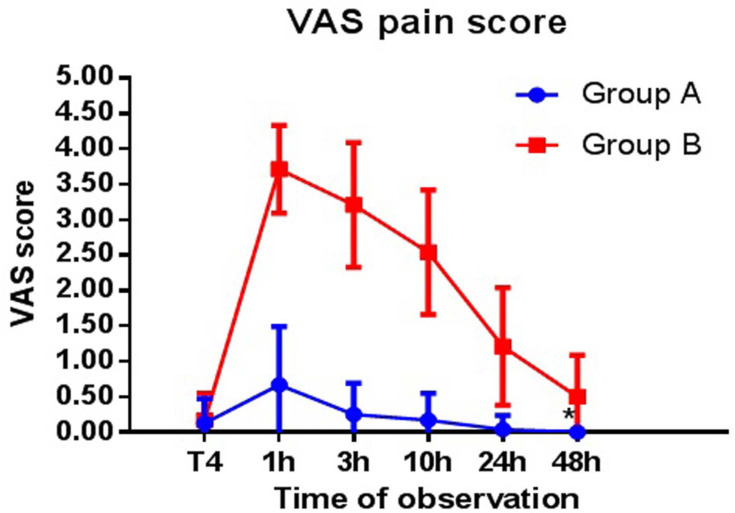
Results: The patients in group A required less remifentanil than group B (2.56±0.92mg vs 3.38±0.84mg, P=0.002) and lower VAS scores at 1, 3, 10, 24, and 48h postoperatively (P < 0.001). While the systolic blood pressure in group A patients was significantly greater than that in group B at T3 (immediately after extubation, [138.33±11.36 vs 129.08±17.06 mmHg; P=0.032]), heart rates in group A were lower than in group B at 1 min before induction (T1 [89.46 ± 9.14 vs 96.71±14.19, P=0.042]) and 1 min after intubation (T2 [70.08 ± 5.35 vs 79.25 ± 11.81, P=0.002]). The extubation time in group A was shorter than that in group B (P < 0.001). There was no difference in calcium, phosphorus and parathormone values, nor in sufentanil consumption between the groups.
Conclusion: Ultrasound-guided bilateral superficial and deep cervical plexus block combined with general anesthesia for TPTA is an effective strategy to improve anesthesia management and achieve better postoperative analgesia, and has no impact on surgical outcomes.
背景:本研究的目的是评估超声引导下双侧颈丛阻滞对甲状旁腺全切除术合并自体移植患者全身麻醉、术后镇痛和手术结果的影响。患者和方法:纳入ASA III-IV级肾衰继发甲状旁腺功能亢进患者48例,超声引导下双侧颈浅、深神经丛阻滞联合全身麻醉24例(A组),单纯全身麻醉24例(B组)。术后患者自控静脉镇痛给予舒芬太尼2 μg/kg。主要结果是术后疼痛评分。次要结局包括术中瑞芬太尼剂量、血流动力学变化、拔管时间和舒芬太尼用量。还记录了手术结果中钙、磷和甲状旁激素的值。结果:A组患者术后1、3、10、24、48h对瑞芬太尼的需药量低于B组(2.56±0.92mg vs 3.38±0.84mg, P=0.002), VAS评分低于B组(P < 0.001)。而A组患者T3(拔管后即刻)收缩压明显高于B组,分别为138.33±11.36 vs 129.08±17.06 mmHg;P=0.032]),诱导前1 min (T1[89.46±9.14比96.71±14.19,P=0.042])和插管后1 min (T2[70.08±5.35比79.25±11.81,P=0.002]) A组心率均低于B组。A组拔管时间明显短于B组(P < 0.001)。两组之间的钙、磷和甲状旁腺激素值没有差异,舒芬太尼的摄入量也没有差异。结论:超声引导下双侧颈浅、深神经丛阻滞联合全身麻醉治疗TPTA是改善麻醉管理、获得较好术后镇痛的有效策略,对手术效果无影响。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
