Incidence, Risk Factors, and Outcomes of Perioperative Atrial Fibrillation following Noncardiothoracic Surgery: A Systematic Review and Meta-Regression Analysis of Observational Studies.
Yamini Subramani, Omar El Tohamy, Daniil Jalali, Mahesh Nagappa, Homer Yang, Ashraf Fayad
{"title":"Incidence, Risk Factors, and Outcomes of Perioperative Atrial Fibrillation following Noncardiothoracic Surgery: A Systematic Review and Meta-Regression Analysis of Observational Studies.","authors":"Yamini Subramani, Omar El Tohamy, Daniil Jalali, Mahesh Nagappa, Homer Yang, Ashraf Fayad","doi":"10.1155/2021/5527199","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrial fibrillation (AF) occurs in 16-30% of patients after cardiac and thoracic surgery and can lead to serious complications like hypoperfusion of vital organs, pulmonary edema, and myocardial infarction. The evidence on risk factors and complications associated with perioperative AF after noncardiothoracic surgery is limited.</p><p><strong>Methods: </strong>The primary objective was to determine demographic and clinical risk factors for new-onset atrial fibrillation associated with noncardiothoracic surgery. A secondary aim was to identify the incidence and odds of perioperative complications associated with the new-onset atrial fibrillation. A systematic search within multiple databases was conducted for studies that explicitly reported on new-onset atrial fibrillation after noncardiothoracic surgery. We reported data on demographics, comorbidities, and perioperative complications as mean difference (MD) or odds ratios (OR) and corresponding 95% confidence interval (CI) using random effects models. A two-sided <i>P</i> value of less than 0.05 was considered significant. We performed meta-regression and sensitivity analysis of various subgroups to confirm the inference of our findings.</p><p><strong>Results: </strong>Eleven studies reporting on 121,517 patients were included, of whom 2,944 developed perioperative AF (incidence rate: 3.7%; 95% CI: 2.3%--6.2%). Advanced age (AF group versus control group: 69.36 ± 10.5 versus 64.37 ± 9.53 years; MD: 4.06; 95% CI: 1.67--6.44; <i>P</i>=0.0009), male gender (52.85% versus 43.59%; OR: 1.08; 95% CI: 0.54 to 1.62; <i>I</i> <sup>2</sup>: 84%; <i>P</i> < 0.0001), preoperative hypertension (60.42% versus 56.51%; OR: 1.15; 95% CI: 1.08 to 1.23; <i>I</i> <sup>2</sup>: 0%; <i>P</i> < 0.00001), diabetes mellitus (22.6% versus 23.04%; OR: 0.97; 95% CI: 0.89 to 1.05; <i>I</i> <sup>2</sup>: 0; <i>P</i> < 0.00001), and cardiac disease (30.64% versus 8.49%; OR: 2.3; 95% CI: 0.28 to 4.31; <i>I</i> <sup>2</sup>: 93%; <i>P</i>=0.03) were found to be significant predictors for perioperative AF. The AF group was at increased odds of developing postoperative cardiac complications (34.1% versus 5%; OR: 5.44; 95% CI: 0.49 to 10.39; <i>I</i> <sup>2</sup>: 82%; <i>P</i>=0.03), postoperative stroke (0.5% versus 0.1%; OR: 3; 95% CI: 0.65 to 5.35; <i>I</i> <sup>2</sup>: 0%; <i>P</i>=0.01), and mortality (7.40% versus 1.92%; OR: 3.58; 95% CI: 0.14 to 7.02; <i>I</i> <sup>2</sup>: 0%; <i>P</i>=0.04). Study quality assessment by meta-regression and sensitivity analysis of the various subgroups did not affect the final inference of the results.</p><p><strong>Conclusion: </strong>We identified advanced age, male gender, preoperative hypertension, diabetes mellitus, and cardiac disease as important risk factors for perioperative atrial fibrillation. The atrial fibrillation group was at increased odds for postoperative cardiac complications, stroke, and higher mortality, emphasizing the need for risk stratification and close monitoring.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2021 ","pages":"5527199"},"PeriodicalIF":1.3000,"publicationDate":"2021-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8099514/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5527199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Atrial fibrillation (AF) occurs in 16-30% of patients after cardiac and thoracic surgery and can lead to serious complications like hypoperfusion of vital organs, pulmonary edema, and myocardial infarction. The evidence on risk factors and complications associated with perioperative AF after noncardiothoracic surgery is limited.
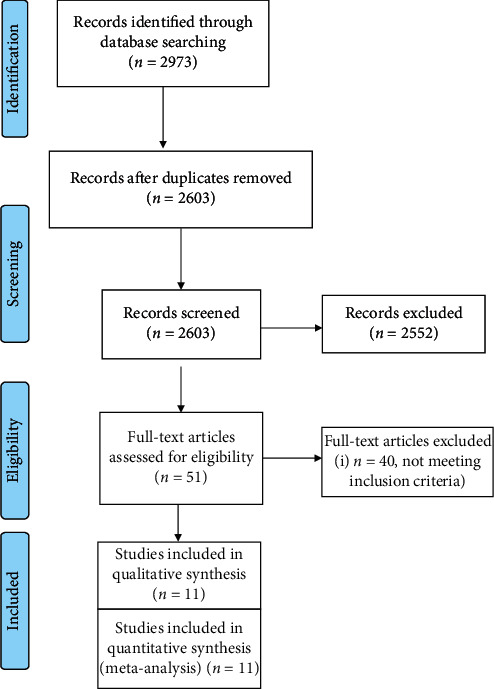
Methods: The primary objective was to determine demographic and clinical risk factors for new-onset atrial fibrillation associated with noncardiothoracic surgery. A secondary aim was to identify the incidence and odds of perioperative complications associated with the new-onset atrial fibrillation. A systematic search within multiple databases was conducted for studies that explicitly reported on new-onset atrial fibrillation after noncardiothoracic surgery. We reported data on demographics, comorbidities, and perioperative complications as mean difference (MD) or odds ratios (OR) and corresponding 95% confidence interval (CI) using random effects models. A two-sided P value of less than 0.05 was considered significant. We performed meta-regression and sensitivity analysis of various subgroups to confirm the inference of our findings.
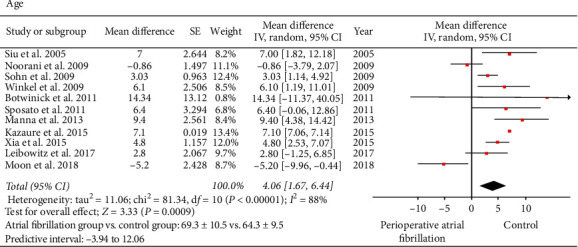
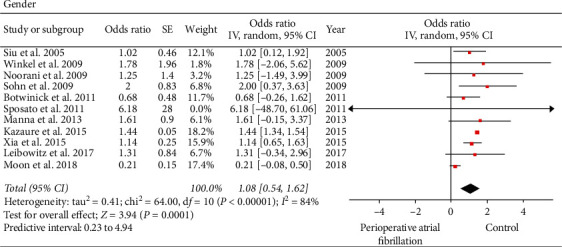
Results: Eleven studies reporting on 121,517 patients were included, of whom 2,944 developed perioperative AF (incidence rate: 3.7%; 95% CI: 2.3%--6.2%). Advanced age (AF group versus control group: 69.36 ± 10.5 versus 64.37 ± 9.53 years; MD: 4.06; 95% CI: 1.67--6.44; P=0.0009), male gender (52.85% versus 43.59%; OR: 1.08; 95% CI: 0.54 to 1.62; I2: 84%; P < 0.0001), preoperative hypertension (60.42% versus 56.51%; OR: 1.15; 95% CI: 1.08 to 1.23; I2: 0%; P < 0.00001), diabetes mellitus (22.6% versus 23.04%; OR: 0.97; 95% CI: 0.89 to 1.05; I2: 0; P < 0.00001), and cardiac disease (30.64% versus 8.49%; OR: 2.3; 95% CI: 0.28 to 4.31; I2: 93%; P=0.03) were found to be significant predictors for perioperative AF. The AF group was at increased odds of developing postoperative cardiac complications (34.1% versus 5%; OR: 5.44; 95% CI: 0.49 to 10.39; I2: 82%; P=0.03), postoperative stroke (0.5% versus 0.1%; OR: 3; 95% CI: 0.65 to 5.35; I2: 0%; P=0.01), and mortality (7.40% versus 1.92%; OR: 3.58; 95% CI: 0.14 to 7.02; I2: 0%; P=0.04). Study quality assessment by meta-regression and sensitivity analysis of the various subgroups did not affect the final inference of the results.
Conclusion: We identified advanced age, male gender, preoperative hypertension, diabetes mellitus, and cardiac disease as important risk factors for perioperative atrial fibrillation. The atrial fibrillation group was at increased odds for postoperative cardiac complications, stroke, and higher mortality, emphasizing the need for risk stratification and close monitoring.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
