Nasogastric- vs. percutaneous gastrostomy tube for prophylactic gastric decompression after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy.
Job P van Kooten, Nadine L de Boer, Marjolein Diepeveen, Cornelis Verhoef, Jacobus W A Burger, Alexandra R M Brandt-Kerkhof, Eva V E Madsen
{"title":"Nasogastric- vs. percutaneous gastrostomy tube for prophylactic gastric decompression after cytoreductive surgery with hyperthermic intraperitoneal chemotherapy.","authors":"Job P van Kooten, Nadine L de Boer, Marjolein Diepeveen, Cornelis Verhoef, Jacobus W A Burger, Alexandra R M Brandt-Kerkhof, Eva V E Madsen","doi":"10.1515/pp-2021-0107","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is associated with postoperative gastroparesis and ileus. In 2015, our practice shifted from using percutaneous gastrostomy tubes (PGT), to nasogastric tubes (NGT) for prophylactic gastric decompression after CRS-HIPEC. This study aimed to compare these methods for length of stay (LOS) and associated complications.</p><p><strong>Methods: </strong>Patients that underwent CRS-HIPEC for peritoneal metastases from colorectal cancer between 2014 and 2019 were included. Cases were grouped based on receiving NGT or PGT postoperatively. Multivariable linear regression determined the independent effect of decompression method on LOS, thereby adjusting for confounders.</p><p><strong>Results: </strong>In total, 179 patients were included in the analyses. Median age was 64 years [IQR:54-71]. Altogether, 135 (75.4%) received a NGT and 44 (24.6%) received a PGT. Gastroparesis occurred significantly more often in the PGT group (18.2 vs. 7.4%, p=0.039). Median LOS was significantly shorter for patients with a NGT (15 [IQR:12-19] vs. 18.5 [IQR:17-25.5], p<0.001). PGT was independently associated with longer LOS in multivariable analysis (Beta=4.224 [95%CI 1.243-7.204]). There was no difference regarding aspiration, pneumonia and postoperative mortality between groups.</p><p><strong>Conclusions: </strong>NGT should be preferred over PGT for gastric decompression after CRS-HIPEC as it is associated with fewer gastroparesis and shorter LOS.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"6 2","pages":"57-65"},"PeriodicalIF":2.4000,"publicationDate":"2021-03-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1515/pp-2021-0107","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2021-0107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/6/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is associated with postoperative gastroparesis and ileus. In 2015, our practice shifted from using percutaneous gastrostomy tubes (PGT), to nasogastric tubes (NGT) for prophylactic gastric decompression after CRS-HIPEC. This study aimed to compare these methods for length of stay (LOS) and associated complications.
Methods: Patients that underwent CRS-HIPEC for peritoneal metastases from colorectal cancer between 2014 and 2019 were included. Cases were grouped based on receiving NGT or PGT postoperatively. Multivariable linear regression determined the independent effect of decompression method on LOS, thereby adjusting for confounders.
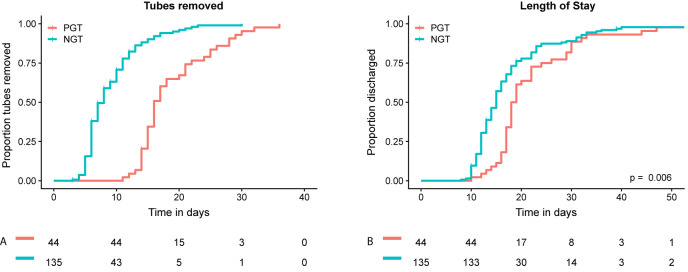
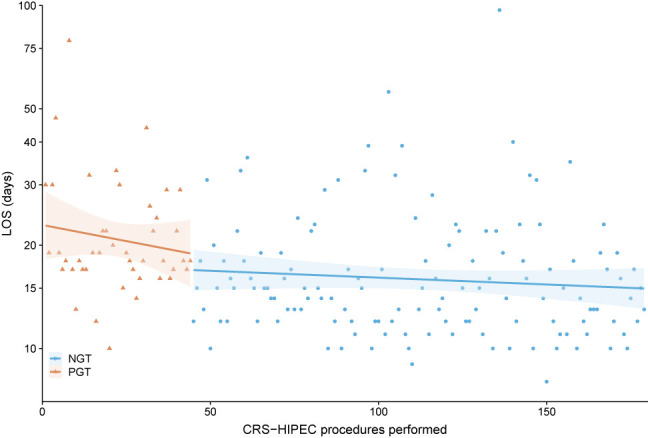
Results: In total, 179 patients were included in the analyses. Median age was 64 years [IQR:54-71]. Altogether, 135 (75.4%) received a NGT and 44 (24.6%) received a PGT. Gastroparesis occurred significantly more often in the PGT group (18.2 vs. 7.4%, p=0.039). Median LOS was significantly shorter for patients with a NGT (15 [IQR:12-19] vs. 18.5 [IQR:17-25.5], p<0.001). PGT was independently associated with longer LOS in multivariable analysis (Beta=4.224 [95%CI 1.243-7.204]). There was no difference regarding aspiration, pneumonia and postoperative mortality between groups.
Conclusions: NGT should be preferred over PGT for gastric decompression after CRS-HIPEC as it is associated with fewer gastroparesis and shorter LOS.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
