Ronald Seidel, Marc Tietke, Oliver Heese, Uwe Walter
{"title":"Serious Complications After Epidural Catheter Placement: Two Case Reports.","authors":"Ronald Seidel, Marc Tietke, Oliver Heese, Uwe Walter","doi":"10.2147/LRA.S324362","DOIUrl":null,"url":null,"abstract":"<p><p>Thoracic epidural analgesia (TEA) is a standard procedure in multimodal analgesia applied in major thoracic and abdominal surgeries. Two cases are presented with serious complications related to TEA. In both cases, earlier reaction of the treating physicians to patient-reported sensory symptoms could have prevented the complicated course. The first case was a 73-year-old patient with bronchial carcinoma who underwent right lower lobe resection. In this case, dabigatran 150 mg/d (indication: permanent atrial fibrillation) had been discontinued 72 hours before surgery, and enoxaparin 80 mg (every 12 hours) had been started 11 hours after surgery. An epidural hematoma developed postoperatively. Magnetic resonance imaging (MRI) was performed only after paraplegia had developed the next day. Unfortunately, delayed hematoma evacuation could not prevent persistent paraplegia in this case, which was complicated by hospital-acquired pneumonia with sepsis and acute renal failure. The second case was a 39-year-old patient with ulcerative colitis and an initially undetected malposition of the epidural catheter. Immediately after test bolus injection, the patient reported paresthesia and overall discomfort, which however could not be safely attributed to either the test dose or the already started general anesthesia. The patient could only be extubated after stopping the epidural infusion. Accidental re-start of epidural infusion led to coma, conjugate eye deviation, and respiratory arrest, necessitating re-intubation. Computed tomography (CT) ruled out intracerebral pathology and showed a catheter position centrally in the spinal canal. Fortunately, no neurological deficits were detected after catheter removal.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"14 ","pages":"117-124"},"PeriodicalIF":1.9000,"publicationDate":"2021-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/87/d4/lra-14-117.PMC8318213.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S324362","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
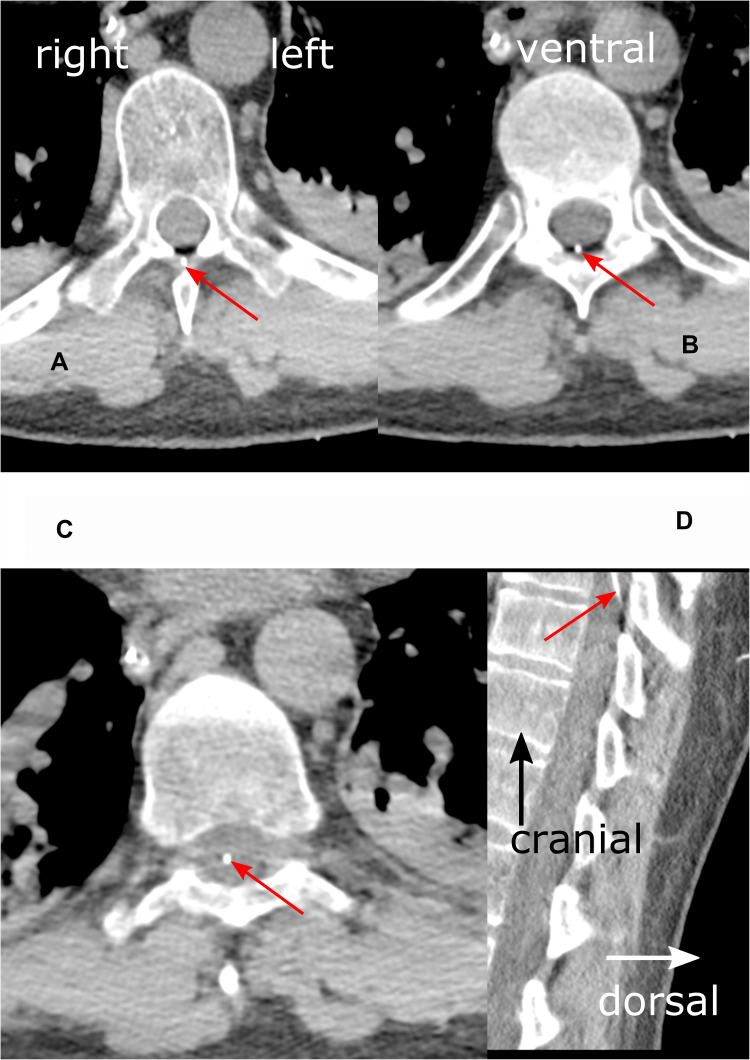
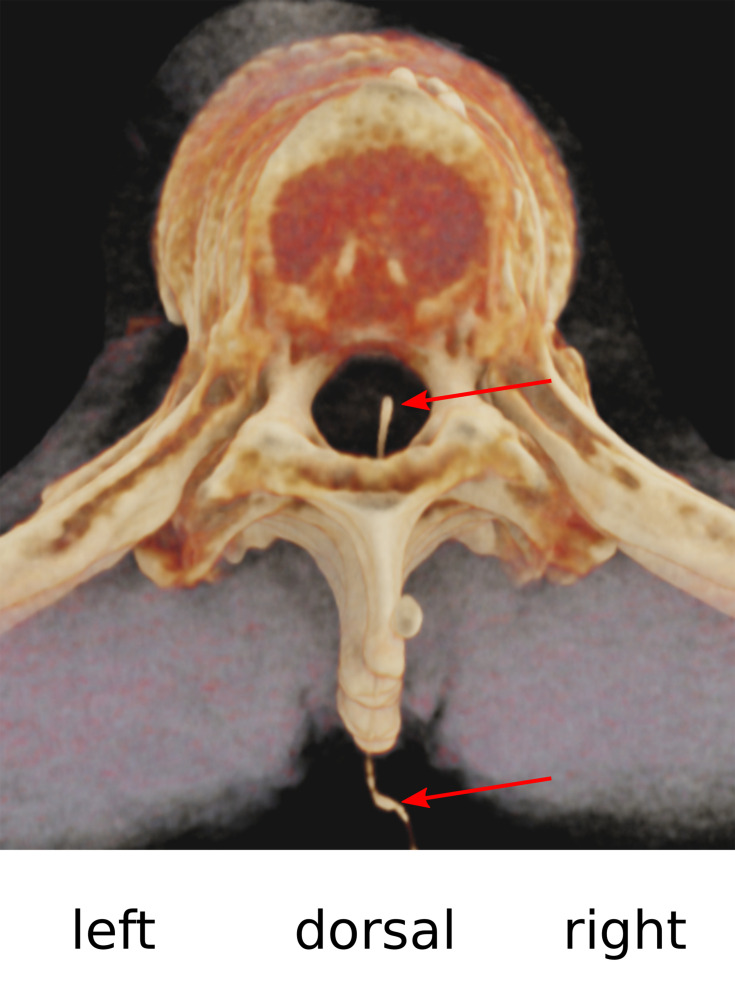
Thoracic epidural analgesia (TEA) is a standard procedure in multimodal analgesia applied in major thoracic and abdominal surgeries. Two cases are presented with serious complications related to TEA. In both cases, earlier reaction of the treating physicians to patient-reported sensory symptoms could have prevented the complicated course. The first case was a 73-year-old patient with bronchial carcinoma who underwent right lower lobe resection. In this case, dabigatran 150 mg/d (indication: permanent atrial fibrillation) had been discontinued 72 hours before surgery, and enoxaparin 80 mg (every 12 hours) had been started 11 hours after surgery. An epidural hematoma developed postoperatively. Magnetic resonance imaging (MRI) was performed only after paraplegia had developed the next day. Unfortunately, delayed hematoma evacuation could not prevent persistent paraplegia in this case, which was complicated by hospital-acquired pneumonia with sepsis and acute renal failure. The second case was a 39-year-old patient with ulcerative colitis and an initially undetected malposition of the epidural catheter. Immediately after test bolus injection, the patient reported paresthesia and overall discomfort, which however could not be safely attributed to either the test dose or the already started general anesthesia. The patient could only be extubated after stopping the epidural infusion. Accidental re-start of epidural infusion led to coma, conjugate eye deviation, and respiratory arrest, necessitating re-intubation. Computed tomography (CT) ruled out intracerebral pathology and showed a catheter position centrally in the spinal canal. Fortunately, no neurological deficits were detected after catheter removal.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
