Ikhwan Rinaldi, Findy Prasetyawaty, Siti Fazlines, Kevin Winston, Yusuf Aji Samudera Nurrobi, Jessica Leoni, Ilham Hidayat Restu Tulus Maha, Satrio Wicaksono, Abdillah Yasir Wicaksono, Averina Octaxena Aslani, Rizkania Ikhsani
{"title":"Diagnosis and Management of Acquired Hemophilia A: Case Reports and a Literature Review.","authors":"Ikhwan Rinaldi, Findy Prasetyawaty, Siti Fazlines, Kevin Winston, Yusuf Aji Samudera Nurrobi, Jessica Leoni, Ilham Hidayat Restu Tulus Maha, Satrio Wicaksono, Abdillah Yasir Wicaksono, Averina Octaxena Aslani, Rizkania Ikhsani","doi":"10.1155/2021/5554664","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acquired hemophilia A (AHA) is a potentially life-threatening autoimmune hemostatic disorder where autoantibodies that disrupt the functions of factor VIII (FVIII) are present in the circulation. The early diagnosis of AHA is difficult since the symptoms of AHA differ from those of congenital hemophilia A. Furthermore, the management of AHA is also more complex due to the presence of autoantibodies against FVIII (FVIII inhibitors). Here, we present three case reports and conduct a literature review of AHA with the aim to increase awareness and knowledge regarding the diagnosis and treatment of AHA. <i>Case Presentations</i>. We present three patients diagnosed with AHA in these case reports. The first patient was a young female, while the second and third patients were middle-aged and elderly males, respectively. All patients presented with a chief complaint of bruises without hemarthrosis and a history of bleeding. Laboratory examinations of the patients revealed isolated prolonged aPTT, normal PT, and the presence of autoantibodies against factor VIII, which are characteristics of AHA. Patients were then treated with corticosteroids to reduce the titer level of autoantibodies and received factor VIII transfusion to stop bleeding.</p><p><strong>Conclusion: </strong>AHA can be suspected in patients presenting with symptoms of bruises without hemarthrosis and without the history of bleeding. Isolated aPTT elevation with normal PT should raise high suspicion of AHA. The presence of FVIII inhibitors can help to confirm the diagnosis of AHA. Treatment consists of factor VIII transfusion and corticosteroid therapy. Bypassing agents are recommended as an alternative to FVIII transfusion.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2021 ","pages":"5554664"},"PeriodicalIF":0.7000,"publicationDate":"2021-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8457949/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5554664","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 1
Abstract
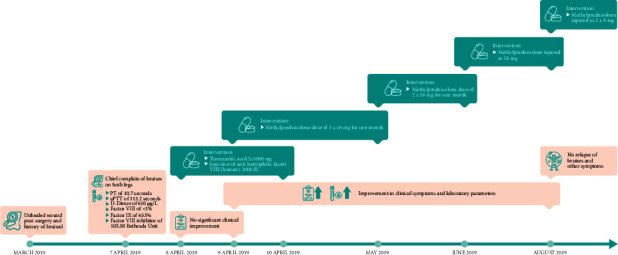
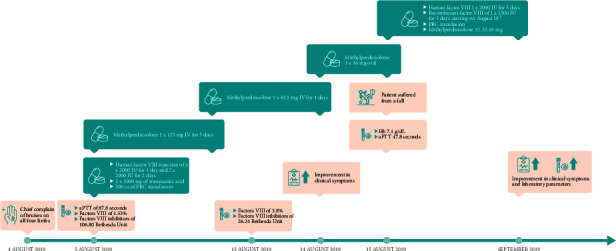
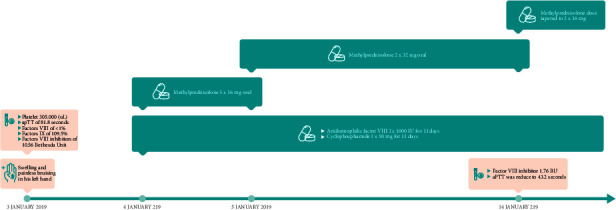
Background: Acquired hemophilia A (AHA) is a potentially life-threatening autoimmune hemostatic disorder where autoantibodies that disrupt the functions of factor VIII (FVIII) are present in the circulation. The early diagnosis of AHA is difficult since the symptoms of AHA differ from those of congenital hemophilia A. Furthermore, the management of AHA is also more complex due to the presence of autoantibodies against FVIII (FVIII inhibitors). Here, we present three case reports and conduct a literature review of AHA with the aim to increase awareness and knowledge regarding the diagnosis and treatment of AHA. Case Presentations. We present three patients diagnosed with AHA in these case reports. The first patient was a young female, while the second and third patients were middle-aged and elderly males, respectively. All patients presented with a chief complaint of bruises without hemarthrosis and a history of bleeding. Laboratory examinations of the patients revealed isolated prolonged aPTT, normal PT, and the presence of autoantibodies against factor VIII, which are characteristics of AHA. Patients were then treated with corticosteroids to reduce the titer level of autoantibodies and received factor VIII transfusion to stop bleeding.
Conclusion: AHA can be suspected in patients presenting with symptoms of bruises without hemarthrosis and without the history of bleeding. Isolated aPTT elevation with normal PT should raise high suspicion of AHA. The presence of FVIII inhibitors can help to confirm the diagnosis of AHA. Treatment consists of factor VIII transfusion and corticosteroid therapy. Bypassing agents are recommended as an alternative to FVIII transfusion.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
