{"title":"Cold Agglutinin Disease.","authors":"Amy P Gabbard, Garrett S Booth","doi":"10.2991/chi.k.200706.001","DOIUrl":null,"url":null,"abstract":"<p><p>Cold agglutinin disease (CAD) is an uncommon form of cold autoimmune hemolytic anemia (AIHA). It should be considered in the differential diagnosis of elderly patients with unexplained chronic anemia presenting with or without cold-induced symptoms in the extremities, such as the fingers, ears, and nose. CAD is a complement-mediated process which leads to intravascular and extravascular hemolysis. A stepwise approach to laboratory testing can help confirm the diagnosis. Nearly all cold agglutinins are positive for the C3d direct antiglobulin test (DAT). A negative C3d DAT should prompt investigation of a possible warm AIHA. Ninety percent of cold agglutinins are of the IgM immunoglobulin class and should have a titer of 1:64 or higher at 4°C. Distinction from a warm AIHA is important, as therapy differs for the two entities. Corticosteroids are not effective at treating CAD and should not be used as therapy in these patients. Approximately 45-60% of patients with CAD respond to rituximab monotherapy. Combination therapy of rituximab and fludarabine has been shown to be effective in up to 76% of patients; however, patients experience more mild side effects with this treatment. New anti-complement drugs, such as eculizumab and sutimlimab, are currently in phase-3 trials to determine their efficacy and safety in patients with CAD.</p>","PeriodicalId":10368,"journal":{"name":"Clinical Hematology International","volume":"2 3","pages":"95-100"},"PeriodicalIF":0.0000,"publicationDate":"2020-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/87/CHI-2-3-95.PMC8432332.pdf","citationCount":"112","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hematology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2991/chi.k.200706.001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 112
Abstract
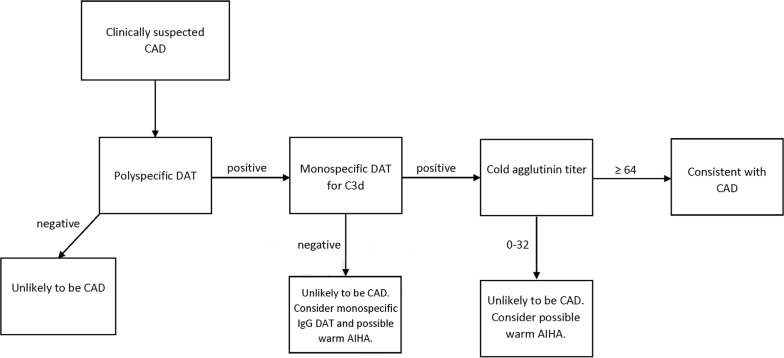
Cold agglutinin disease (CAD) is an uncommon form of cold autoimmune hemolytic anemia (AIHA). It should be considered in the differential diagnosis of elderly patients with unexplained chronic anemia presenting with or without cold-induced symptoms in the extremities, such as the fingers, ears, and nose. CAD is a complement-mediated process which leads to intravascular and extravascular hemolysis. A stepwise approach to laboratory testing can help confirm the diagnosis. Nearly all cold agglutinins are positive for the C3d direct antiglobulin test (DAT). A negative C3d DAT should prompt investigation of a possible warm AIHA. Ninety percent of cold agglutinins are of the IgM immunoglobulin class and should have a titer of 1:64 or higher at 4°C. Distinction from a warm AIHA is important, as therapy differs for the two entities. Corticosteroids are not effective at treating CAD and should not be used as therapy in these patients. Approximately 45-60% of patients with CAD respond to rituximab monotherapy. Combination therapy of rituximab and fludarabine has been shown to be effective in up to 76% of patients; however, patients experience more mild side effects with this treatment. New anti-complement drugs, such as eculizumab and sutimlimab, are currently in phase-3 trials to determine their efficacy and safety in patients with CAD.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
