Telemedicine monitoring of high-risk coronavirus disease 2019 (COVID-19) patients by family medicine service after discharge from the emergency department.
Imran Khalid, Maryam Imran, Manahil Imran, Saifullah Khan, Muhammad A Akhtar, Khadijah Amanullah, Tabindeh J Khalid
{"title":"Telemedicine monitoring of high-risk coronavirus disease 2019 (COVID-19) patients by family medicine service after discharge from the emergency department.","authors":"Imran Khalid, Maryam Imran, Manahil Imran, Saifullah Khan, Muhammad A Akhtar, Khadijah Amanullah, Tabindeh J Khalid","doi":"10.4103/jfcm.jfcm_184_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Up to 25% of the total coronavirus disease 2019 (COVID-19) admissions comprise patients with comorbidities who present to the emergency department (ED) with only mild-to-moderate disease. It is unclear whether as an alternative to hospitalization, telemedicine can be used to monitor these \"high-risk\" comorbid patients. The aim of our study was to answer this question by comparing the outcome of such patients discharged under a family medicine service (FMS) telemonitoring program and those admitted to hospital.</p><p><strong>Materials and methods: </strong>Patients with three or more risk factors for progression to severe COVID-19 disease were designated as \"high-risk\" in our study. In the absence of acute indication for hospitalization, these high-risk patients with mild-to-moderate disease were discharged home under the supervision of FMS led telemonitoring between October 2020 and February 2021 and were labelled as \"Telemedicine group.\" They were compared to similar patients who were admitted to hospital between March-August 2020 before the implementation of telemedicine service (TMS) and were taken as \"Control group.\" Outcome measures included intubation, number of inpatient days, 28-day mortality and cost analysis for the two groups.</p><p><strong>Results: </strong>Out of 572 COVID-19 patients who presented to the ED, 70 met the inclusion criteria for the \"Telemedicine Group\" and 35 were included in the \"Control Group\". In the Telemedicine group, 21 (30.0%) patients were brought back to ED for re-evaluation and 16 (22.9%) were eventually admitted to the hospital. There was no difference in terms of oxygen requirements, intubation, and intensive care unit admission (<i>P</i> > 0.74) between the groups, and none of the study patients died. The Family Medicine-led TMS saved 77% inpatient admissions and on average 4.4 hospital days and $3400 per patient (<i>P</i> < . 0001).</p><p><strong>Conclusion: </strong>Family medicine-led telemonitoring of high-risk COVID-19 patients presenting to the ED with mild-to-moderate disease is a feasible and cost-effective alternative to hospitalization.</p>","PeriodicalId":46862,"journal":{"name":"Journal of Family and Community Medicine","volume":"28 3","pages":"210-216"},"PeriodicalIF":1.7000,"publicationDate":"2021-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e6/8b/JFCM-28-210.PMC8496702.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Family and Community Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jfcm.jfcm_184_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Up to 25% of the total coronavirus disease 2019 (COVID-19) admissions comprise patients with comorbidities who present to the emergency department (ED) with only mild-to-moderate disease. It is unclear whether as an alternative to hospitalization, telemedicine can be used to monitor these "high-risk" comorbid patients. The aim of our study was to answer this question by comparing the outcome of such patients discharged under a family medicine service (FMS) telemonitoring program and those admitted to hospital.
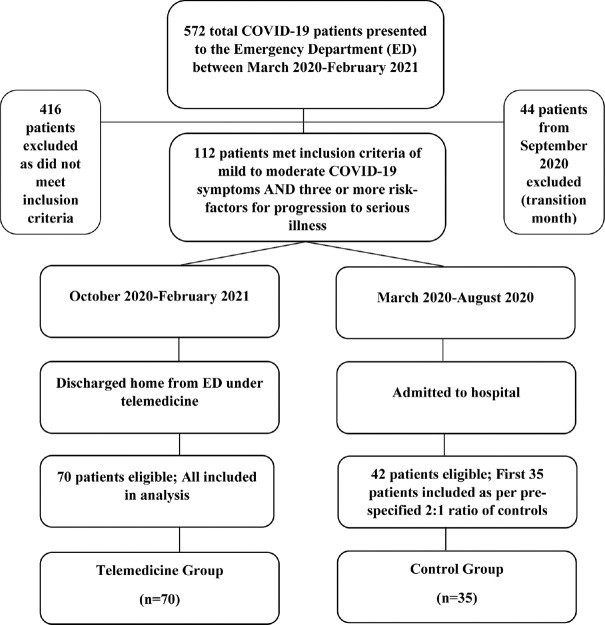
Materials and methods: Patients with three or more risk factors for progression to severe COVID-19 disease were designated as "high-risk" in our study. In the absence of acute indication for hospitalization, these high-risk patients with mild-to-moderate disease were discharged home under the supervision of FMS led telemonitoring between October 2020 and February 2021 and were labelled as "Telemedicine group." They were compared to similar patients who were admitted to hospital between March-August 2020 before the implementation of telemedicine service (TMS) and were taken as "Control group." Outcome measures included intubation, number of inpatient days, 28-day mortality and cost analysis for the two groups.
Results: Out of 572 COVID-19 patients who presented to the ED, 70 met the inclusion criteria for the "Telemedicine Group" and 35 were included in the "Control Group". In the Telemedicine group, 21 (30.0%) patients were brought back to ED for re-evaluation and 16 (22.9%) were eventually admitted to the hospital. There was no difference in terms of oxygen requirements, intubation, and intensive care unit admission (P > 0.74) between the groups, and none of the study patients died. The Family Medicine-led TMS saved 77% inpatient admissions and on average 4.4 hospital days and $3400 per patient (P < . 0001).
Conclusion: Family medicine-led telemonitoring of high-risk COVID-19 patients presenting to the ED with mild-to-moderate disease is a feasible and cost-effective alternative to hospitalization.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
