Kyungmann Kim, Charles H Hennekens, Lisa Martinez, J Michael Gaziano, Marc A Pfeffer, Bianca Biglione, Alexander Gitin, Jeanne Bell McCabe, Thomas D Cook, David L DeMets, Sarah K Wood
{"title":"Primary care providers should prescribe aspirin to prevent cardiovascular disease based on benefit-risk ratio, not age.","authors":"Kyungmann Kim, Charles H Hennekens, Lisa Martinez, J Michael Gaziano, Marc A Pfeffer, Bianca Biglione, Alexander Gitin, Jeanne Bell McCabe, Thomas D Cook, David L DeMets, Sarah K Wood","doi":"10.1136/fmch-2021-001475","DOIUrl":null,"url":null,"abstract":"<p><p>Recent guidelines restricted aspirin (ASA) in primary prevention of cardiovascular disease (CVD) to patients <70 years old and more recent guidance to <60.In the most comprehensive prior meta-analysis, the Antithrombotic Trialists Collaboration reported a significant 12% reduction in CVD with similar benefit-risk ratios at older ages. Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, four trials were added to an updated meta-analysis.ASA produced a statistically significant 13% reduction in CVD with 95% confidence limits (0.83 to 0.92) with similar benefits at older ages in each of the trials.Primary care providers should make individual decisions whether to prescribe ASA based on benefit-risk ratio, not simply age. When the absolute risk of CVD is >10%, benefits of ASA will generally outweigh risks of significant bleeding. ASA should be considered only after implementation of therapeutic lifestyle changes and other drugs of proven benefit such as statins, which are, at the very least, additive to ASA. Our perspective is that individual clinical judgements by primary care providers about prescription of ASA in primary prevention of CVD should be based on our evidence-based solution of weighing all the absolute benefits and risks rather than age. This strategy would do far more good for far more patients as well as far more good than harm in both developed and developing countries. This new and novel strategy for primary care providers to consider in prescribing ASA in primary prevention of CVD is the same as the general approach suggested by Professor Geoffrey Rose decades ago.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"9 4","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2021-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f8/f0/fmch-2021-001475.PMC8710906.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2021-001475","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
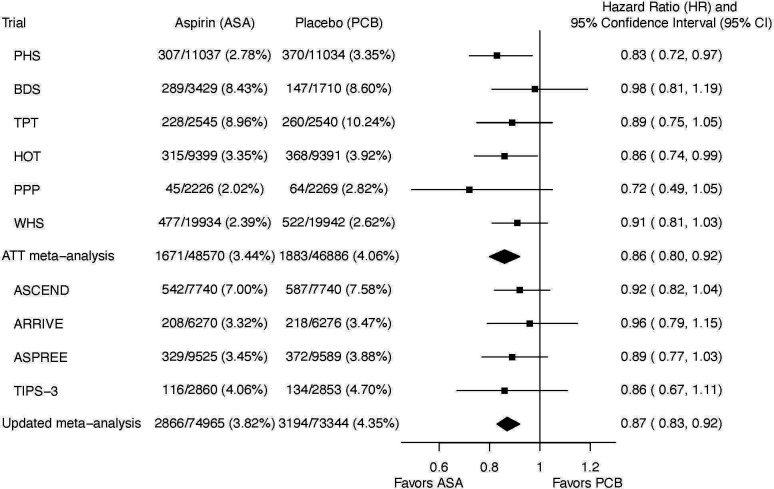
Recent guidelines restricted aspirin (ASA) in primary prevention of cardiovascular disease (CVD) to patients <70 years old and more recent guidance to <60.In the most comprehensive prior meta-analysis, the Antithrombotic Trialists Collaboration reported a significant 12% reduction in CVD with similar benefit-risk ratios at older ages. Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, four trials were added to an updated meta-analysis.ASA produced a statistically significant 13% reduction in CVD with 95% confidence limits (0.83 to 0.92) with similar benefits at older ages in each of the trials.Primary care providers should make individual decisions whether to prescribe ASA based on benefit-risk ratio, not simply age. When the absolute risk of CVD is >10%, benefits of ASA will generally outweigh risks of significant bleeding. ASA should be considered only after implementation of therapeutic lifestyle changes and other drugs of proven benefit such as statins, which are, at the very least, additive to ASA. Our perspective is that individual clinical judgements by primary care providers about prescription of ASA in primary prevention of CVD should be based on our evidence-based solution of weighing all the absolute benefits and risks rather than age. This strategy would do far more good for far more patients as well as far more good than harm in both developed and developing countries. This new and novel strategy for primary care providers to consider in prescribing ASA in primary prevention of CVD is the same as the general approach suggested by Professor Geoffrey Rose decades ago.
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
