Rene Aleman, David Gutierrez Blanco, David Romero Funes, Lisandro Montorfano, George Semien, Samuel Szomstein, Emanuele Lo Menzo, Raul J Rosenthal
{"title":"Does Transverse Abdominis Plane Block Increase the Risk of Postoperative Urinary Retention after Inguinal Hernia Repair?","authors":"Rene Aleman, David Gutierrez Blanco, David Romero Funes, Lisandro Montorfano, George Semien, Samuel Szomstein, Emanuele Lo Menzo, Raul J Rosenthal","doi":"10.4293/JSLS.2021.00015","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Postoperative urinary retention (POUR) is a common adverse event after inguinal hernia repair (IHR), with an incidence of up to 22.2%. The aim of this study is to determine if pre-operative transverse abdominis plane (TAP) block increases the incidence of POUR.</p><p><strong>Methods: </strong>A retrospective review was performed for all patients who underwent IHR (open or laparoscopic) at this institution, from January 1, 2016 to December 31, 2017. Patients were divided into two groups: Patients that had a TAP block before surgery (group 1) and patients with no TAP block (group 2). Common demographics and comorbidities were collected along with postoperative outcomes and POUR incidence rates for every group to determine procedural influence.</p><p><strong>Results: </strong>From 276 patients reviewed, 28.2% (N = 78) underwent TAP block before surgery. The patient cohort mean age was 61.1 ± 14.4 years. Most the interventions were laparoscopic (81.2%) and an overall POUR incidence rate of 7.6% (N = 21) was observed. Comparatively, common demographics and comorbidities were statistically similar for both groups, with the exception of type 2 diabetes mellitus (<i>p </i>=<i> </i>0.049). Individually, group 1 and 2 presented POUR incidence rates of 14.1% and 5.05%, respectively. While intraoperative fluid administration, early readmission rate, and length were similar in both groups, there was a significant difference in POUR incidence rates (<i>p </i>=<i> </i>0.01).</p><p><strong>Conclusion: </strong>Patients undergoing TAP block during IHR might have an increased risk of developing POUR. Further larger, prospective, and randomized controlled studies are necessary to better assess these findings.</p>","PeriodicalId":17679,"journal":{"name":"JSLS : Journal of the Society of Laparoendoscopic Surgeons","volume":"25 4","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/86/17/e2021.00015.PMC8580164.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JSLS : Journal of the Society of Laparoendoscopic Surgeons","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4293/JSLS.2021.00015","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 3
Abstract
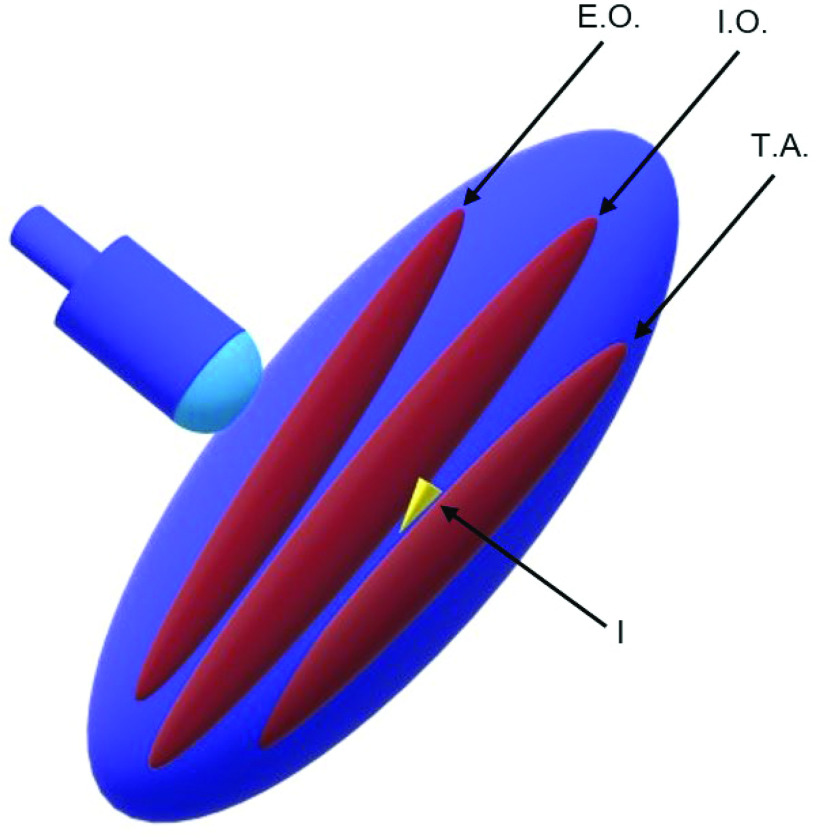
Background and objective: Postoperative urinary retention (POUR) is a common adverse event after inguinal hernia repair (IHR), with an incidence of up to 22.2%. The aim of this study is to determine if pre-operative transverse abdominis plane (TAP) block increases the incidence of POUR.
Methods: A retrospective review was performed for all patients who underwent IHR (open or laparoscopic) at this institution, from January 1, 2016 to December 31, 2017. Patients were divided into two groups: Patients that had a TAP block before surgery (group 1) and patients with no TAP block (group 2). Common demographics and comorbidities were collected along with postoperative outcomes and POUR incidence rates for every group to determine procedural influence.
Results: From 276 patients reviewed, 28.2% (N = 78) underwent TAP block before surgery. The patient cohort mean age was 61.1 ± 14.4 years. Most the interventions were laparoscopic (81.2%) and an overall POUR incidence rate of 7.6% (N = 21) was observed. Comparatively, common demographics and comorbidities were statistically similar for both groups, with the exception of type 2 diabetes mellitus (p =0.049). Individually, group 1 and 2 presented POUR incidence rates of 14.1% and 5.05%, respectively. While intraoperative fluid administration, early readmission rate, and length were similar in both groups, there was a significant difference in POUR incidence rates (p =0.01).
Conclusion: Patients undergoing TAP block during IHR might have an increased risk of developing POUR. Further larger, prospective, and randomized controlled studies are necessary to better assess these findings.
期刊介绍:
JSLS, Journal of the Society of Laparoscopic & Robotic Surgeons publishes original scientific articles on basic science and technical topics in all the fields involved with laparoscopic, robotic, and minimally invasive surgery. CRSLS, MIS Case Reports from SLS is dedicated to the publication of Case Reports in the field of minimally invasive surgery. The journals seek to advance our understandings and practice of minimally invasive, image-guided surgery by providing a forum for all relevant disciplines and by promoting the exchange of information and ideas across specialties.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
