Crystal A. West , Steven D. Beck , Shyama M.E. Masilamani
{"title":"Time course of renal sodium transport in the pregnant rat","authors":"Crystal A. West , Steven D. Beck , Shyama M.E. Masilamani","doi":"10.1016/j.crphys.2021.10.001","DOIUrl":null,"url":null,"abstract":"<div><p>Progressive sodium retention and cumulative plasma volume expansion occur to support the developing fetus during pregnancy. Sodium retention is regulated by individual tubular transporters and channels. An increase or decrease in any single transporter could cause a change in sodium balance. Understanding the time-course for changes in each sodium transporter during pregnancy will enable us to understand progressive sodium retention seen in pregnancy. Here, we examined the activity of the major apical sodium transporters found in the nephron using natriuretic response tests in virgin, early pregnant, mid-pregnant, and late pregnant rats. We also measured renal and serum aldosterone levels. We found that furosemide sensitive sodium transport (NKCC2) is only increased during late pregnancy, thiazide sensitive sodium transport (NDCBE/pendrin) is increased in all stages of pregnancy, and that benzamil sensitive sodium transport (ENaC) is increased beginning in mid-pregnancy. We also found that serum aldosterone levels progressively increased throughout gestation and kidney tissue aldosterone levels increased only during late pregnancy. Here we have shown progressive turning on of specific sodium transport mechanisms to help support progressive sodium retention through the course of gestation. These mechanisms contribute to the renal sodium retention and plasma volume expansion required for an optimal pregnancy.</p></div>","PeriodicalId":72753,"journal":{"name":"Current research in physiology","volume":"4 ","pages":"Pages 229-234"},"PeriodicalIF":1.7000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/fe/main.PMC8710989.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current research in physiology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2665944121000274","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHYSIOLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
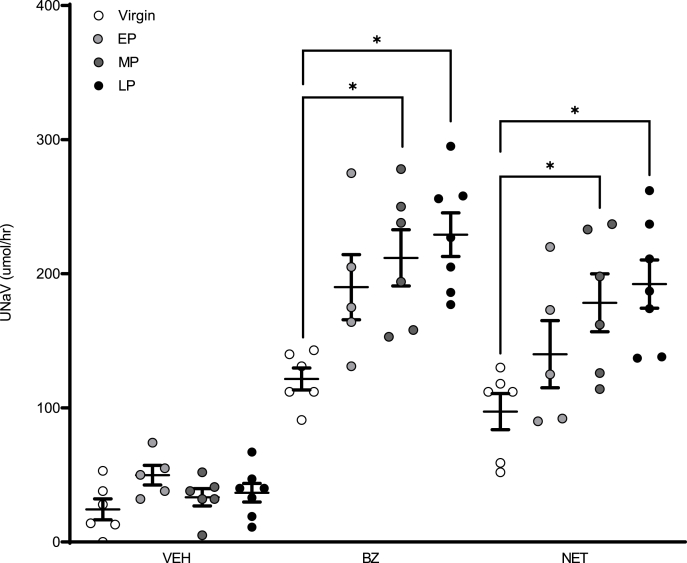
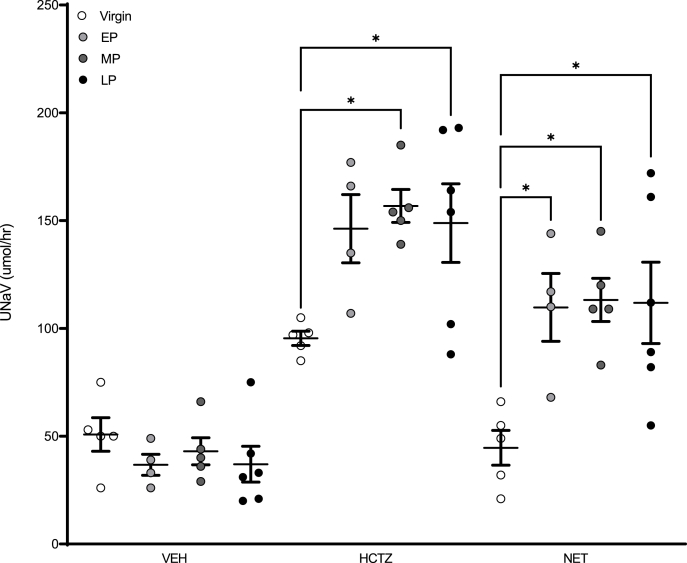
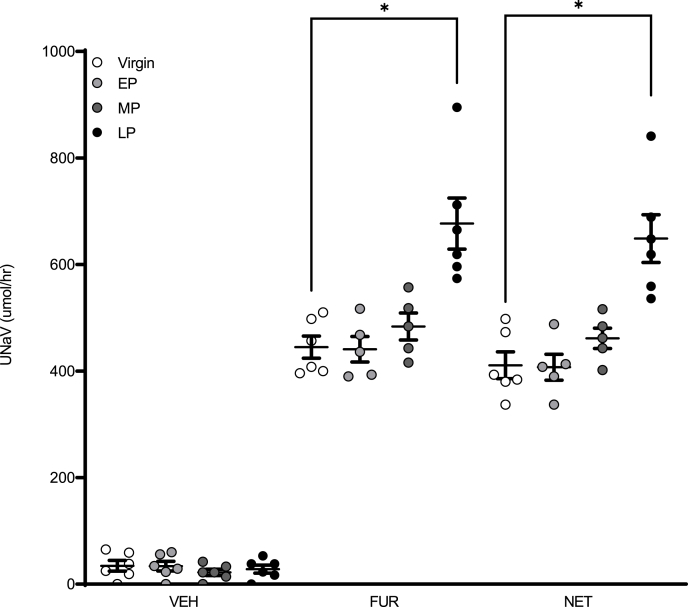
Progressive sodium retention and cumulative plasma volume expansion occur to support the developing fetus during pregnancy. Sodium retention is regulated by individual tubular transporters and channels. An increase or decrease in any single transporter could cause a change in sodium balance. Understanding the time-course for changes in each sodium transporter during pregnancy will enable us to understand progressive sodium retention seen in pregnancy. Here, we examined the activity of the major apical sodium transporters found in the nephron using natriuretic response tests in virgin, early pregnant, mid-pregnant, and late pregnant rats. We also measured renal and serum aldosterone levels. We found that furosemide sensitive sodium transport (NKCC2) is only increased during late pregnancy, thiazide sensitive sodium transport (NDCBE/pendrin) is increased in all stages of pregnancy, and that benzamil sensitive sodium transport (ENaC) is increased beginning in mid-pregnancy. We also found that serum aldosterone levels progressively increased throughout gestation and kidney tissue aldosterone levels increased only during late pregnancy. Here we have shown progressive turning on of specific sodium transport mechanisms to help support progressive sodium retention through the course of gestation. These mechanisms contribute to the renal sodium retention and plasma volume expansion required for an optimal pregnancy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
