Xianglin L Du, Lara M Simpson, Brian C Tandy, Judy Bettencourt, Barry R Davis
{"title":"Effects of Posttrial Antihypertensive Drugs on Morbidity and Mortality: Findings from 15-Year Passive Follow-Up after ALLHAT Ended.","authors":"Xianglin L Du, Lara M Simpson, Brian C Tandy, Judy Bettencourt, Barry R Davis","doi":"10.1155/2021/2261144","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) ended in 2002, but it is important to study its long-term outcomes during the posttrial period by incorporating posttrial antihypertensive medication uses in the analysis.</p><p><strong>Purposes: </strong>The primary aim is to explore the patterns of antihypertensive medication use during the posttrial period from Medicare Part-D data over the 11-year period from 2007 to 2017. The secondary aim is to examine the potential effects of these posttrial antihypertensive medications on the observed mortality and morbidity benefits.</p><p><strong>Methods: </strong>This is a posttrial passive follow-up study of ALLHAT participants in 567 US centers in 1994-1998 with the last date of active in-trial follow-up on March 31, 2002, by linking with their Medicare and National Death Index data through 2017 among 8,007 subjects receiving antihypertensive drugs (3,637 for chlorthalidone, 2,189 for amlodipine, and 2,181 for lisinopril). Outcomes included posttrial antihypertensive drug use, all-cause mortality, and cardiovascular disease (CVD) mortality.</p><p><strong>Results: </strong>Of 8007 subjects, 3,637 participants were initially randomized to diuretic (chlorthalidone). The majority (67.9%) of them still received diuretics in 2007, and 52.7%, 47.2%, and 44.0% received <i>β</i>-blockers, angiotensin-converting enzyme (ACE) inhibitors, and calcium channel blockers (CCBs), respectively. Compared to participants who received diuretic-based antihypertensives, those who received CCB had a nonsignificantly higher risk of all-cause mortality (1.17, 0.99-1.37), whereas those who received ACE/ARB (angiotensin receptor blockers) had a significantly higher risk of all-cause mortality (1.26, 1.09-1.45). For the combined fatal or nonfatal hospitalized events, the risk of CVD was significantly higher in patients receiving CCB (1.30, 1.04-1.61) and ACE/ARB (1.49, 1.22-1.81) as compared to patients receiving diuretics.</p><p><strong>Conclusion: </strong>After the conclusion of the ALLHAT, almost all patients switched to combination antihypertensive therapies, independently by the original drug class, and the combination therapies (mostly based on diuretics) reduced the incidence of major cardiovascular outcomes and mortality.</p>","PeriodicalId":14132,"journal":{"name":"International Journal of Hypertension","volume":"2021 ","pages":"2261144"},"PeriodicalIF":1.7000,"publicationDate":"2021-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8677412/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Hypertension","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2021/2261144","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) ended in 2002, but it is important to study its long-term outcomes during the posttrial period by incorporating posttrial antihypertensive medication uses in the analysis.
Purposes: The primary aim is to explore the patterns of antihypertensive medication use during the posttrial period from Medicare Part-D data over the 11-year period from 2007 to 2017. The secondary aim is to examine the potential effects of these posttrial antihypertensive medications on the observed mortality and morbidity benefits.
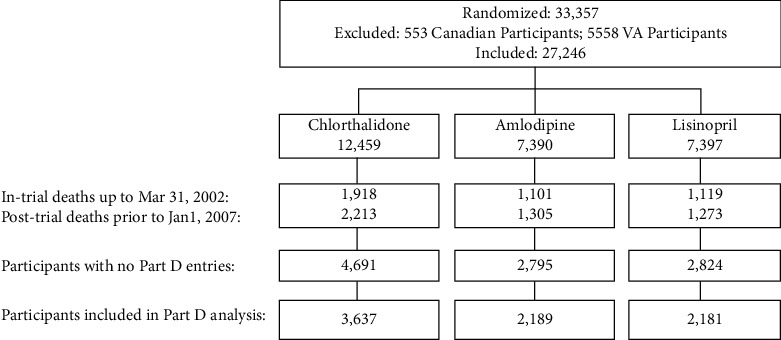
Methods: This is a posttrial passive follow-up study of ALLHAT participants in 567 US centers in 1994-1998 with the last date of active in-trial follow-up on March 31, 2002, by linking with their Medicare and National Death Index data through 2017 among 8,007 subjects receiving antihypertensive drugs (3,637 for chlorthalidone, 2,189 for amlodipine, and 2,181 for lisinopril). Outcomes included posttrial antihypertensive drug use, all-cause mortality, and cardiovascular disease (CVD) mortality.
Results: Of 8007 subjects, 3,637 participants were initially randomized to diuretic (chlorthalidone). The majority (67.9%) of them still received diuretics in 2007, and 52.7%, 47.2%, and 44.0% received β-blockers, angiotensin-converting enzyme (ACE) inhibitors, and calcium channel blockers (CCBs), respectively. Compared to participants who received diuretic-based antihypertensives, those who received CCB had a nonsignificantly higher risk of all-cause mortality (1.17, 0.99-1.37), whereas those who received ACE/ARB (angiotensin receptor blockers) had a significantly higher risk of all-cause mortality (1.26, 1.09-1.45). For the combined fatal or nonfatal hospitalized events, the risk of CVD was significantly higher in patients receiving CCB (1.30, 1.04-1.61) and ACE/ARB (1.49, 1.22-1.81) as compared to patients receiving diuretics.
Conclusion: After the conclusion of the ALLHAT, almost all patients switched to combination antihypertensive therapies, independently by the original drug class, and the combination therapies (mostly based on diuretics) reduced the incidence of major cardiovascular outcomes and mortality.
期刊介绍:
International Journal of Hypertension is a peer-reviewed, Open Access journal that provides a forum for clinicians and basic scientists interested in blood pressure regulation and pathophysiology, as well as treatment and prevention of hypertension. The journal publishes original research articles, review articles, and clinical studies on the etiology and risk factors of hypertension, with a special focus on vascular biology, epidemiology, pediatric hypertension, and hypertensive nephropathy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
