Harshavardhan Rao B, Priya Nair, Anoop K Koshy, S Krishnapriya, C R Greeshma, Rama P Venu
{"title":"Role of High-Density Lipoprotein Cholesterol (HDL-C) as a Clinical Predictor of Decompensation in Patients with Chronic Liver Disease (CLD).","authors":"Harshavardhan Rao B, Priya Nair, Anoop K Koshy, S Krishnapriya, C R Greeshma, Rama P Venu","doi":"10.1155/2021/1795851","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Systemic inflammation triggered by bacterial products like lipopolysaccharides (LPS) in the circulation is an important factor leading to decompensation in patients with chronic liver disease (CLD). High-density lipoprotein cholesterol (HDL-C) has a significant role in innate immune response to LPS in the circulation and could therefore increase the risk for decompensation in patients with CLD. In this study, we have explored the role of HDL-C as a prognostic marker for decompensation.</p><p><strong>Methods: </strong>This was a prospective, observational, cohort study where consecutive patients with CLD were included. Patients with cholestatic liver disease and hepatocellular carcinoma were excluded. Fasting lipids were measured in all patients at the time of recruitment. Each patient was carefully followed up for development of decompensation events such as new-onset/worsening ascites, hepatic encephalopathy, or variceal bleed during follow-up.</p><p><strong>Results: </strong>A total of 170 patients were included (mean age 60 ± 11.5 years, M : F = 6 : 1). At the end of follow-up, 97/170 patients (57%) had decompensation events. Mean HDL-C levels were significantly lower among patients with decompensation (27.5 ± 15 mg/dL vs. 43.5 ± 13.9 mg/dL; <i>p</i> value 0.004). Using ROC analysis, cut-off for HDL-C of 36.4 mg/dL was identified. On multivariate analysis, HDL-C (OR = 6.072; 95% CI 2.39-15.39) was found to have an independent association with risk of decompensation.</p><p><strong>Conclusions: </strong>HDL-C level (<36.4 mg/dL) is a reliable marker for risk of decompensation and can be a useful addition to existing prognostic scoring systems in CLD. It can be a valuable tool to streamline treatment protocols and prioritise liver transplantation.</p>","PeriodicalId":46297,"journal":{"name":"International Journal of Hepatology","volume":"2021 ","pages":"1795851"},"PeriodicalIF":1.4000,"publicationDate":"2021-12-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8720002/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/1795851","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Systemic inflammation triggered by bacterial products like lipopolysaccharides (LPS) in the circulation is an important factor leading to decompensation in patients with chronic liver disease (CLD). High-density lipoprotein cholesterol (HDL-C) has a significant role in innate immune response to LPS in the circulation and could therefore increase the risk for decompensation in patients with CLD. In this study, we have explored the role of HDL-C as a prognostic marker for decompensation.
Methods: This was a prospective, observational, cohort study where consecutive patients with CLD were included. Patients with cholestatic liver disease and hepatocellular carcinoma were excluded. Fasting lipids were measured in all patients at the time of recruitment. Each patient was carefully followed up for development of decompensation events such as new-onset/worsening ascites, hepatic encephalopathy, or variceal bleed during follow-up.
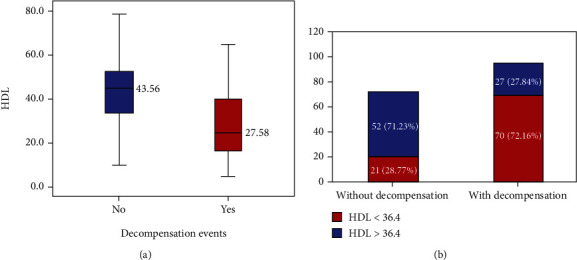
Results: A total of 170 patients were included (mean age 60 ± 11.5 years, M : F = 6 : 1). At the end of follow-up, 97/170 patients (57%) had decompensation events. Mean HDL-C levels were significantly lower among patients with decompensation (27.5 ± 15 mg/dL vs. 43.5 ± 13.9 mg/dL; p value 0.004). Using ROC analysis, cut-off for HDL-C of 36.4 mg/dL was identified. On multivariate analysis, HDL-C (OR = 6.072; 95% CI 2.39-15.39) was found to have an independent association with risk of decompensation.
Conclusions: HDL-C level (<36.4 mg/dL) is a reliable marker for risk of decompensation and can be a useful addition to existing prognostic scoring systems in CLD. It can be a valuable tool to streamline treatment protocols and prioritise liver transplantation.
由循环中脂多糖(LPS)等细菌产物引发的全身性炎症是导致慢性肝病(CLD)患者代偿失调的重要因素。高密度脂蛋白胆固醇(HDL-C)在循环中对LPS的先天免疫反应中起重要作用,因此可能增加CLD患者代偿失调的风险。在这项研究中,我们探讨了HDL-C作为失代偿预后标志物的作用。方法:这是一项前瞻性、观察性、队列研究,包括连续的CLD患者。排除了胆汁淤积性肝病和肝细胞癌患者。在招募时测量所有患者的空腹血脂。在随访期间,对每位患者进行仔细随访,以了解失代偿事件的发展情况,如新发/恶化的腹水、肝性脑病或静脉曲张出血。结果:共纳入170例患者(平均年龄60±11.5岁,M: F = 6: 1),随访结束时,170例患者中有97例(57%)发生失代偿事件。失代偿患者的平均HDL-C水平显著降低(27.5±15 mg/dL vs. 43.5±13.9 mg/dL;P值0.004)。采用ROC分析,确定HDL-C的临界值为36.4 mg/dL。多因素分析,HDL-C (OR = 6.072;95% CI 2.39-15.39)与失代偿风险独立相关。结论:HDL-C水平(
期刊介绍:
International Journal of Hepatology is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies related to the medical, surgical, pathological, biochemical, and physiological aspects of hepatology, as well as the management of disorders affecting the liver, gallbladder, biliary tree, and pancreas.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
