Maria Månsson Martinez, Lampros Spiliopoulos, Falastin Salami, Daniel Agardh, Jorma Toppari, Åke Lernmark, Jukka Kero, Riitta Veijola, Päivi Tossavainen, Sauli Palmu, Markus Lundgren, Henrik Borg, Anastasia Katsarou, Helena Elding Larsson, Mikael Knip, Marlena Maziarz, Carina Törn
{"title":"Heterogeneity of beta-cell function in subjects with multiple islet autoantibodies in the TEDDY family prevention study - TEFA.","authors":"Maria Månsson Martinez, Lampros Spiliopoulos, Falastin Salami, Daniel Agardh, Jorma Toppari, Åke Lernmark, Jukka Kero, Riitta Veijola, Päivi Tossavainen, Sauli Palmu, Markus Lundgren, Henrik Borg, Anastasia Katsarou, Helena Elding Larsson, Mikael Knip, Marlena Maziarz, Carina Törn","doi":"10.1186/s40842-021-00135-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Individuals with multiple islet autoantibodies are at increased risk for clinical type 1 diabetes and may proceed gradually from stage to stage complicating the recruitment to secondary prevention studies. We evaluated multiple islet autoantibody positive subjects before randomisation for a clinical trial 1 month apart for beta-cell function, glucose metabolism and continuous glucose monitoring (CGM). We hypothesized that the number and type of islet autoantibodies in combination with different measures of glucose metabolism including fasting glucose, HbA1c, oral glucose tolerance test (OGTT), intra venous glucose tolerance test (IvGTT) and CGM allows for more precise staging of autoimmune type 1 diabetes than the number of islet autoantibodies alone.</p><p><strong>Methods: </strong>Subjects (n = 57) at 2-50 years of age, positive for two or more islet autoantibodies were assessed by fasting plasma insulin, glucose, HbA1c as well as First Phase Insulin Response (FPIR) in IvGTT, followed 1 month later by OGTT, and 1 week of CGM (n = 24).</p><p><strong>Results: </strong>Autoantibodies against GAD65 (GADA; n = 52), ZnT8 (ZnT8A; n = 40), IA-2 (IA-2A; n = 38) and insulin (IAA; n = 28) were present in 9 different combinations of 2-4 autoantibodies. Fasting glucose and HbA1c did not differ between the two visits. The estimate of the linear relationship between log2-transformed FPIR as the outcome and log2-transformed area under the OGTT glucose curve (AUC) as the predictor, adjusting for age and sex was - 1.88 (- 2.71, - 1.05) p = 3.49 × 10-5. The direction of the estimates for all glucose metabolism measures was positive except for FPIR, which was negative. FPIR was associated with higher blood glucose. Both the median and the spread of the CGM glucose data were significantly associated with higher glucose values based on OGTT, higher HbA1c, and lower FPIR. There was no association between glucose metabolism, autoantibody number and type except that there was an indication that the presence of at least one of ZnT8(Q/R/W) A was associated with a lower log2-transformed FPIR (- 0.80 (- 1.58, - 0.02), p = 0.046).</p><p><strong>Conclusions: </strong>The sole use of two or more islet autoantibodies as inclusion criterion for Stage 1 diabetes in prevention trials is unsatisfactory. Staging type 1 diabetes needs to take the heterogeneity in beta-cell function and glucose metabolism into account.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov identifier: NCT02605148 , November 16, 2015.</p>","PeriodicalId":56339,"journal":{"name":"Clinical Diabetes and Endocrinology","volume":"7 1","pages":"23"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8728995/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Diabetes and Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40842-021-00135-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Individuals with multiple islet autoantibodies are at increased risk for clinical type 1 diabetes and may proceed gradually from stage to stage complicating the recruitment to secondary prevention studies. We evaluated multiple islet autoantibody positive subjects before randomisation for a clinical trial 1 month apart for beta-cell function, glucose metabolism and continuous glucose monitoring (CGM). We hypothesized that the number and type of islet autoantibodies in combination with different measures of glucose metabolism including fasting glucose, HbA1c, oral glucose tolerance test (OGTT), intra venous glucose tolerance test (IvGTT) and CGM allows for more precise staging of autoimmune type 1 diabetes than the number of islet autoantibodies alone.
Methods: Subjects (n = 57) at 2-50 years of age, positive for two or more islet autoantibodies were assessed by fasting plasma insulin, glucose, HbA1c as well as First Phase Insulin Response (FPIR) in IvGTT, followed 1 month later by OGTT, and 1 week of CGM (n = 24).
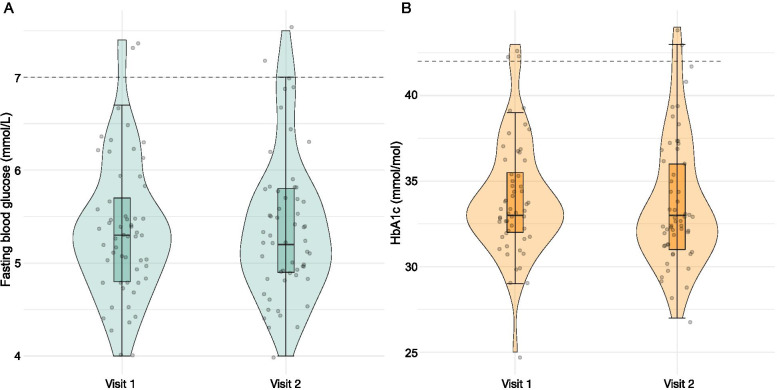
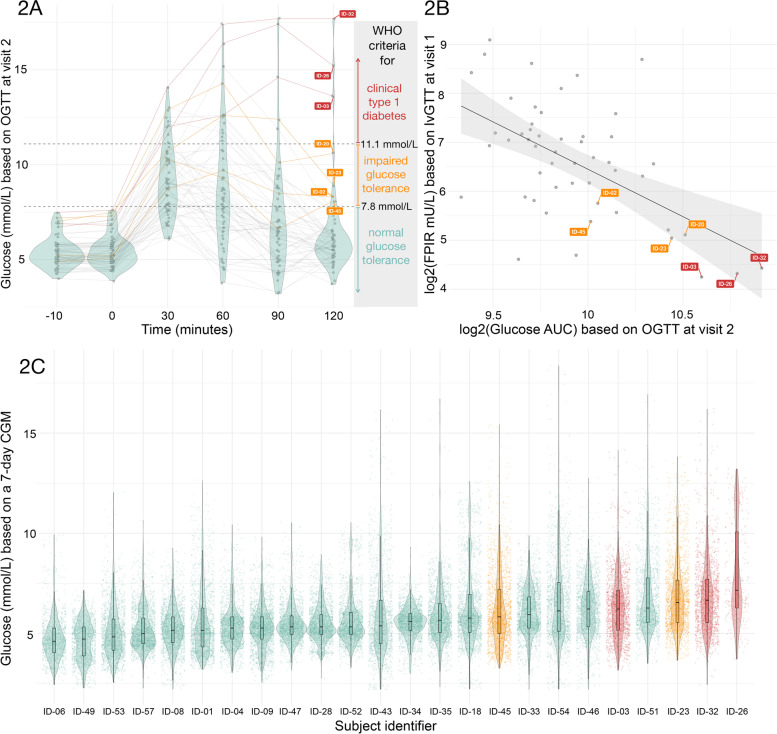
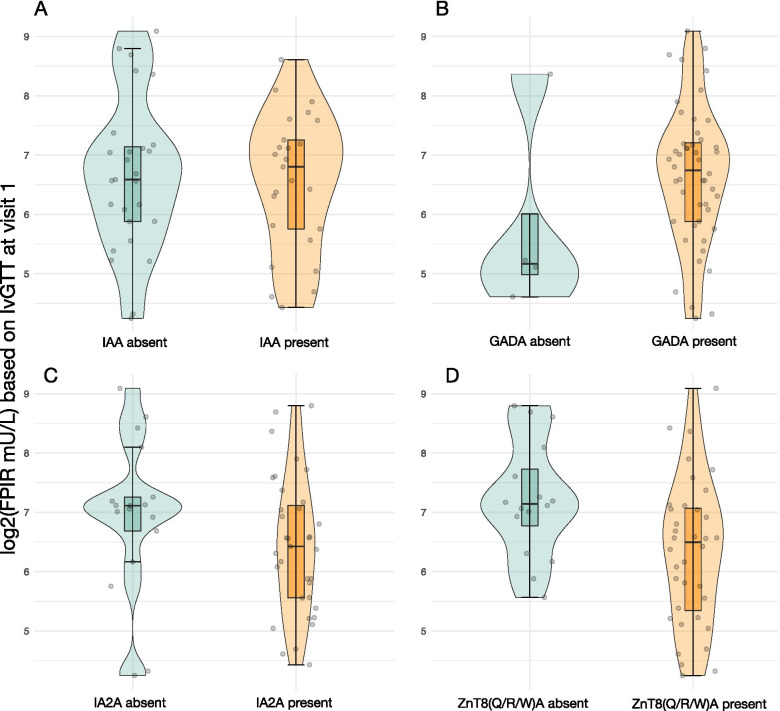
Results: Autoantibodies against GAD65 (GADA; n = 52), ZnT8 (ZnT8A; n = 40), IA-2 (IA-2A; n = 38) and insulin (IAA; n = 28) were present in 9 different combinations of 2-4 autoantibodies. Fasting glucose and HbA1c did not differ between the two visits. The estimate of the linear relationship between log2-transformed FPIR as the outcome and log2-transformed area under the OGTT glucose curve (AUC) as the predictor, adjusting for age and sex was - 1.88 (- 2.71, - 1.05) p = 3.49 × 10-5. The direction of the estimates for all glucose metabolism measures was positive except for FPIR, which was negative. FPIR was associated with higher blood glucose. Both the median and the spread of the CGM glucose data were significantly associated with higher glucose values based on OGTT, higher HbA1c, and lower FPIR. There was no association between glucose metabolism, autoantibody number and type except that there was an indication that the presence of at least one of ZnT8(Q/R/W) A was associated with a lower log2-transformed FPIR (- 0.80 (- 1.58, - 0.02), p = 0.046).
Conclusions: The sole use of two or more islet autoantibodies as inclusion criterion for Stage 1 diabetes in prevention trials is unsatisfactory. Staging type 1 diabetes needs to take the heterogeneity in beta-cell function and glucose metabolism into account.
Trial registration: ClinicalTrials.gov identifier: NCT02605148 , November 16, 2015.
期刊介绍:
Clinical Diabetes and Endocrinology is an open access journal publishing within the field of diabetes and endocrine disease. The journal aims to provide a widely available resource for people working within the field of diabetes and endocrinology, in order to improve the care of people affected by these conditions. The audience includes, but is not limited to, physicians, researchers, nurses, nutritionists, pharmacists, podiatrists, psychologists, epidemiologists, exercise physiologists and health care researchers. Research articles include patient-based research (clinical trials, clinical studies, and others), translational research (translation of basic science to clinical practice, translation of clinical practice to policy and others), as well as epidemiology and health care research. Clinical articles include case reports, case seminars, consensus statements, clinical practice guidelines and evidence-based medicine. Only articles considered to contribute new knowledge to the field will be considered for publication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
